
Central Nervous System Lymphoma
Overview
Central nervous system lymphoma is a type of cancer that affects the central nervous system (CNS), which consists of the brain and spinal cord. This type of lymphoma forms when white blood cells called lymphocytes develop mutations, multiply uncontrollably in the CNS, and become malignant or cancerous.
All central nervous system lymphomas (CNS lymphomas) are considered rare forms of non-Hodgkin lymphoma and fall into one of two categories:
- Primary CNS lymphoma (PCNSL): As the more common form of CNS lymphoma, PCSNL occurs when cancer cells form in the brain, spinal cord, or eyes but do not spread to other parts of the body.
- Secondary CNS lymphoma: This type of lymphoma is rare and happens when lymphoma starts elsewhere in the body, like the lymph nodes, and then spreads to the central nervous system.
What causes central nervous system lymphoma?
While the cause of cancerous lymphocytes in the central nervous system is not fully understood, multiple factors can contribute to their growth.
A weakened or compromised immune system is the first and foremost culprit. When the immune system isn’t functioning as intended, malignant lymphocytes have an opportunity to grow exponentially and form tumors.
A compromised immune system is most often caused by one of the following:
- HIV and AIDS: People with HIV or AIDS are at a significantly higher risk of developing CNS lymphoma, as HIV and AIDS weaken the immune system and, as a result, make it less effective at controlling abnormal cell growth.
- Long-term immunosuppression: Autoimmune diseases like lupus or rheumatoid arthritis, as well as medications used to suppress the immune system, increase the risk of developing CNS lymphoma. What’s more, the longer someone is on immunosuppressive therapy, the higher their risk for developing CNS lymphoma.
- Organ transplant recipients: After an organ transplant, doctors prescribe immunosuppressive medications to prevent the body from rejecting the new organ. These medications lower the immune system’s ability to fight infections and control abnormal cell growth, increasing the risk of cancers like CNS lymphoma.
- Inherited immune deficiencies: People born with certain genetic conditions that affect the immune system, like Wiskott-Aldrich syndrome or severe combined immunodeficiency (SCID), are also at a higher risk for CNS lymphoma.
Outside of a compromised immune system, other known risk factors for CNS lymphoma include:
- Epstein-Barr virus (EBV): The virus that causes mononucleosis—colloquially known as mono—has been linked to an increased risk of CNS lymphoma. Scientists think EBV infection causes the condition by triggering an abnormal growth of lymphocytes, especially in those with compromised immune systems.
- Older age: CNS lymphoma is more common in adults over 60. In general, susceptibility to abnormal cell growth increases with age as the immune system weakens.
In some cases, CNS lymphoma happens in people with no identifiable risk factors. While these cases aren’t as common, research is ongoing to understand why a small percentage of people without known risk factors develop the condition.

CNS Lymphoma Symptoms
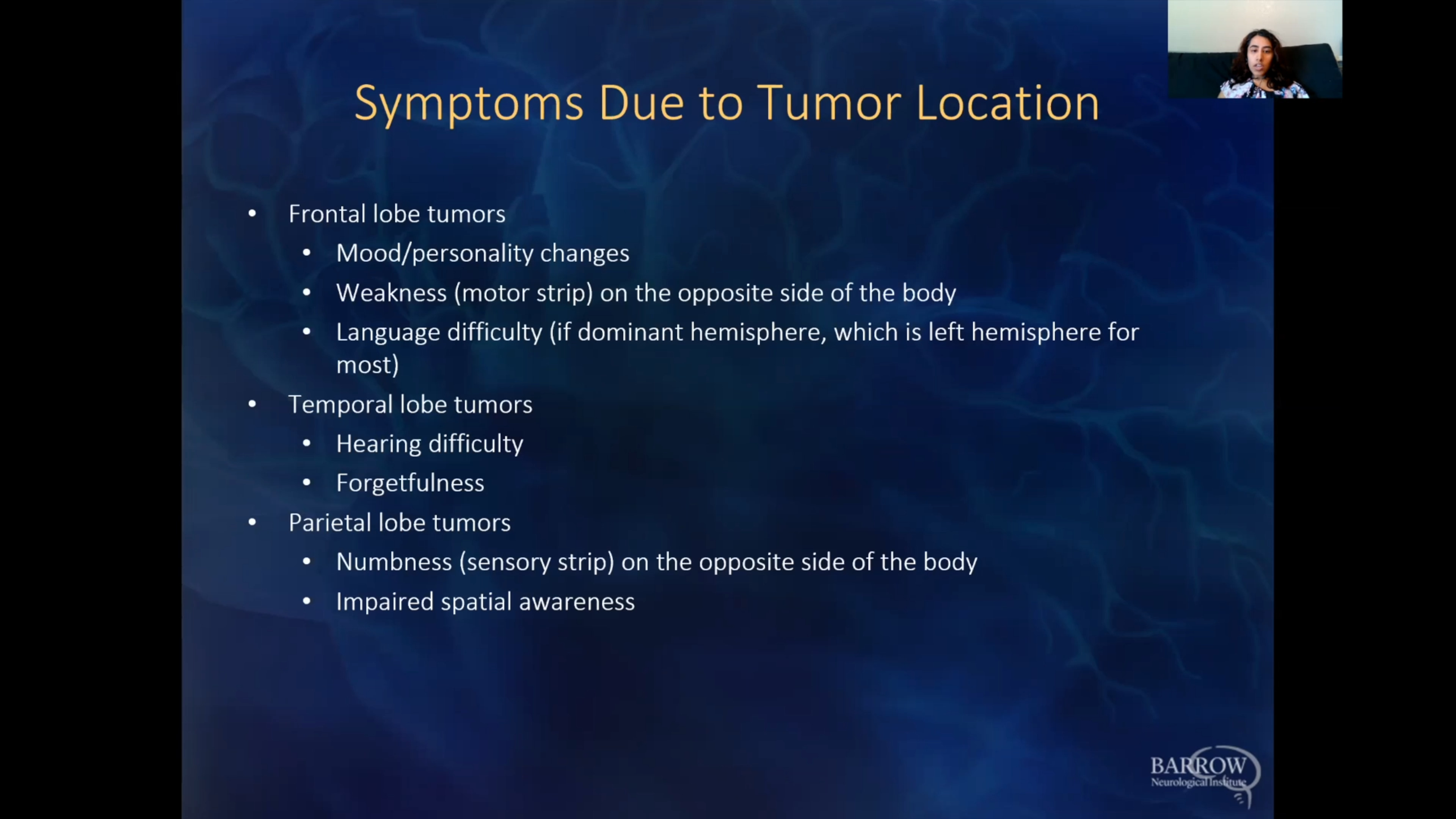
The symptoms of central nervous system lymphoma (CNS lymphoma) vary depending on where in the body it is growing and whether it exerts pressure on the brain, spinal cord, or eyes.
Symptoms you might notice if you or someone you know has a CNS lymphoma can include:
- Headaches: Persistent headaches are among the most common early symptoms, generally due to increased pressure inside the skull. Your headaches may worsen over time and not respond well to treatments that have worked for you in the past, like over-the-counter pain relievers.
- Weakness or paralysis: Because a CNS lymphoma presses on the brain or spinal cord, it can cause muscle weakness in the legs or numbness or tingling in the extremities, especially on one side of the body.
- Seizures: Some people develop new seizures that can manifest as sudden muscle spasms, involuntary movements, or loss of consciousness.
- Behavioral changes: Personality changes like becoming withdrawn or aggressive, feeling emotionally unstable, experiencing slowed thinking or disorientation, and having trouble making decisions can occur as the parts of the brain that control your emotions and behavior are affected by lymphoma growth.
- Drowsiness or difficulty staying awake: As a lymphoma grows, the increased pressure inside your skull can prompt unusual drowsiness and mental status changes, like becoming less alert.
- Balance and coordination problems: When a lymphoma affects the part of the brain responsible for movement, trouble walking or a loss of coordination can occur.
- Nausea or vomiting: Increased pressure in the brain can lead to nausea or vomiting, which can be worse in the morning.
- Vision problems: Up to 20% of patients with CNS lymphoma develop an eye cancer known as ocular lymphoma. Symptoms of ocular lymphoma can include blurred or double vision, eye pain, partial or complete loss of vision, and sensitivity to light.
If you’re concerned about any new or persistent symptoms that align with those outlined above, it’s critical you talk to your healthcare provider to schedule an evaluation as soon as possible. Early diagnosis and treatment are crucial to managing CNS lymphoma and preventing complications.
Diagnosis
Diagnosing central nervous system lymphoma (CNS lymphoma) involves multiple steps to determine the extent of the condition. Your healthcare provider will use a combination of imaging studies, laboratory tests, and occasionally more invasive procedures to make the most accurate diagnosis.
The most common diagnostic tests for CNS lymphoma include:
- Physical and neurological exam: First, your provider will begin by reviewing your symptoms, medical history, and any risk factors you may have, like a weakened immune system. Next, your provider will conduct a neurological examination to check your vision, coordination, reflexes, strength, and other functions controlled by the brain and spinal cord.
- Magnetic Resonance Imaging (MRI): Imaging studies are crucial in visualizing the brain and identifying abnormalities. An MRI provides detailed brain images and can help determine a tumor’s location, size, and characteristics.
- Computed Tomography (CT): CT scans rely on X-rays to create detailed cross-sectional images of the brain and the rest of the body, helping to detect tumors while evaluating their size and location.
- Biopsy: A biopsy establishes an exact tumor diagnosis by removing a small tissue sample from the tumor surgically or through stereotactic biopsy. Neuropathologists then examine the tissue under a microscope to determine the type of cells present and other important characteristics that will guide treatment decisions.
- Lumbar puncture: Also known as a spinal tap, a lumbar puncture involves a needle inserted into the lower back to collect cerebrospinal fluid (CSF). This fluid surrounds the brain and spinal cord and is tested for the presence of lymphoma cells. If lymphoma cells are detected in the CSF, it can confirm the diagnosis and identify if cancer has metastasized to the spinal cord. Medical professionals can also test cerebrospinal fluid for proteins or markers associated with CNS lymphoma.
- Blood tests: Your care team will use blood tests to assess your overall health and check for any abnormalities associated with CNS lymphoma. A complete blood count will check for your number of red blood cells and platelets, your number and type of white blood cells, the amount of hemoglobin in your red blood cells, and the portion of the sample made up of red blood cells.
- Eye exam: If you’re experiencing vision changes, an eye exam that includes a sample of the fluid or tissue from inside your eye may be done to determine if any lymphoma cells have spread to your eyes.
- Positron Emission Tomography (PET) scan: PET scans evaluate the metabolic activity of brain tumors and lymphomas in other organs to determine their aggressiveness. They’re also occasionally used to determine whether a lymphoma exists outside of the central nervous system.
Once a number of these tests have been completed, your providers will use the results to confirm a diagnosis and the extent of the disease in your central nervous system. In some cases, the biopsy or fluid sample testing for specific genetic mutations or other markers can provide information about the type of lymphoma and help guide your treatment plan.

CNS Lymphoma Treatment
Central nervous system lymphoma (CNS lymphoma) is a high-grade, aggressive lymphoma that requires timely treatment to minimize damage to your central nervous system.
While there is no single course of treatment, treatment generally follows two phases:
- Phase I: Phase I treatments, or remission induction therapy, aim to target all the lymphoma seen on scans to achieve remission.
- Phase II: Phase II treatments, or consolidation therapy, aim to destroy any lymphoma cells left behind, stopping the lymphoma from returning and keeping it under control for as long as possible.
Nonsurgical Treatments
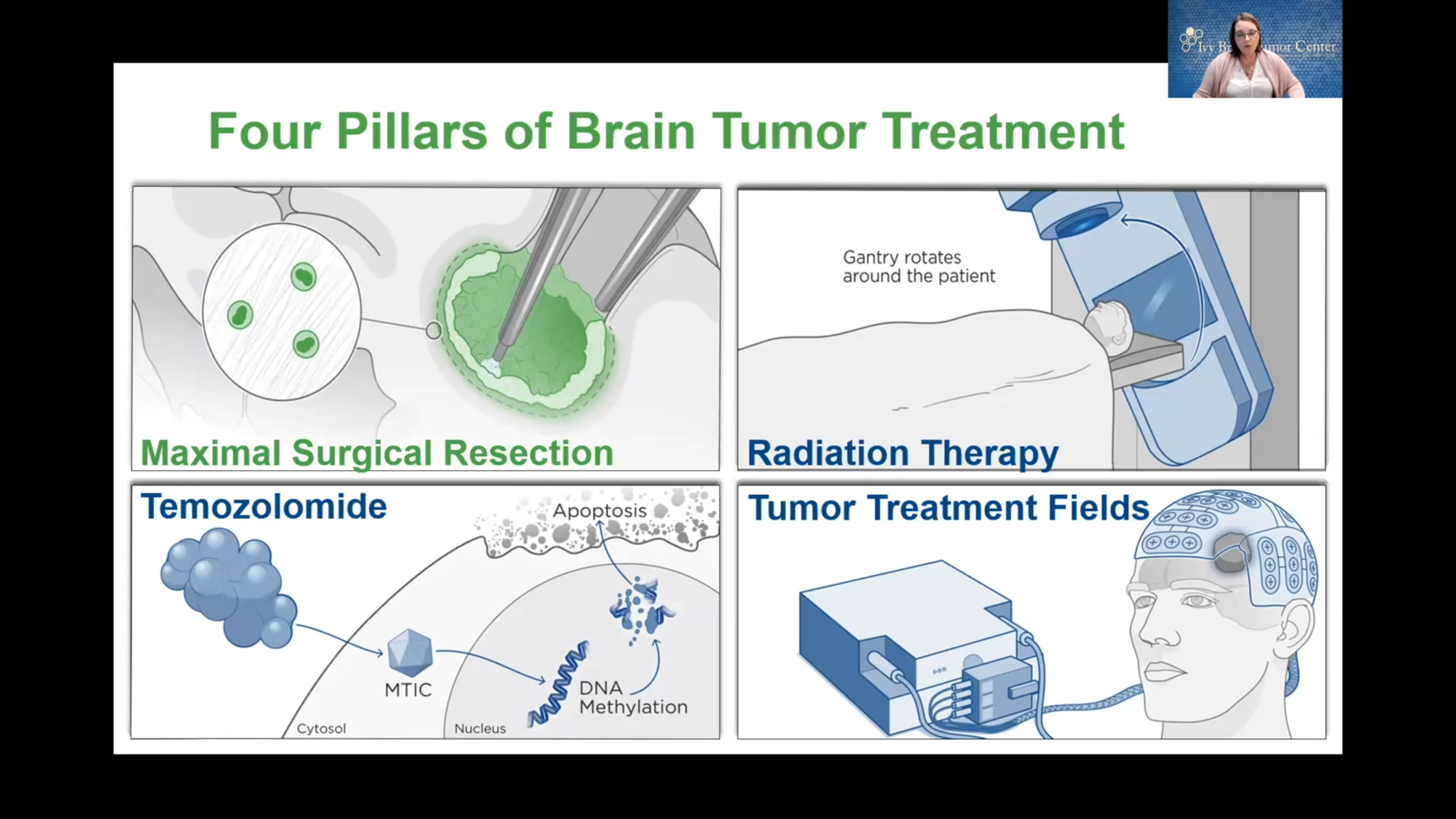
Treatment for CNS lymphoma generally involves nonsurgical therapies, like chemotherapy and radiation, because surgery is not nearly as safe or effective for this type of lymphoma.
- Chemotherapy: Given orally or intravenously, chemotherapy drugs inhibit the growth of cancer cells and effectively bring about remission in many patients, especially if your lymphoma is caught early and chemotherapy is used in combination with radiation therapy or surgery. Sometimes chemotherapy is administered intrathecally, or injected directly into the cerebrospinal fluid (CSF). This is because the blood-brain barrier—the protective layer around the brain—can prevent medications taken orally or intravenously from reaching the central nervous system. The most commonly used chemotherapy drug is high-dose methotrexate, as it can cross the blood-brain barrier.
- Ocular chemotherapy or radiation: If CNS lymphoma involves the eyes, your physician can prescribe intraocular chemotherapy, which is delivered directly into the eye, or local radiation to the eyes can be used to target lymphoma cells. Typically, intravenous methotrexate is effective.
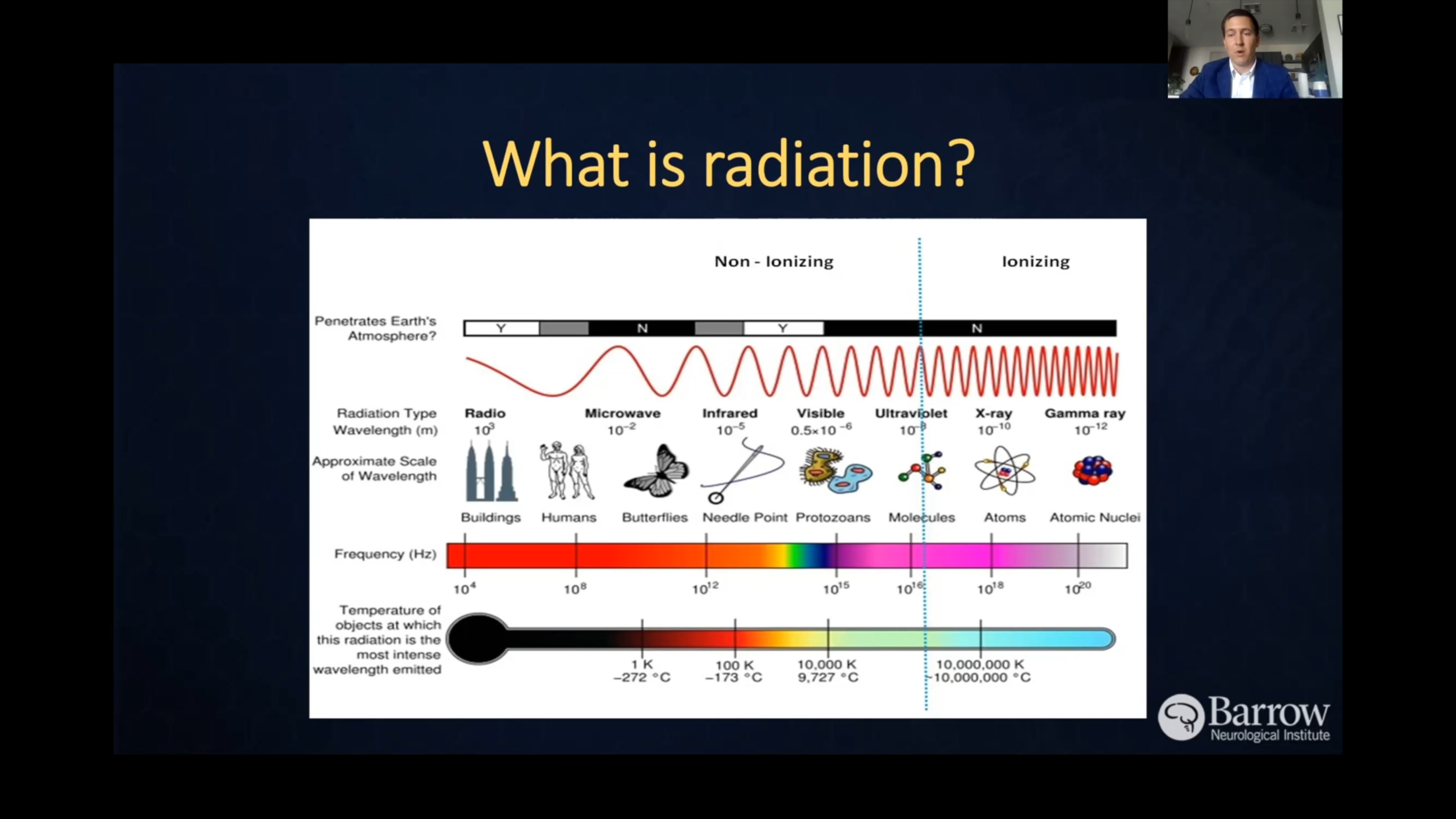
- Radiation therapy: Radiation therapy uses precisely aimed beams of radiation to destroy tumors in the body. While it doesn’t remove the tumor, radiation therapy damages the DNA of the tumor cells, which then lose their ability to reproduce and eventually die. Doctors routinely use radiation as a second-line treatment in conjunction with chemotherapy.
- Targeted therapy: Targeted therapy uses compounds to target specific molecules vital to cancer cells’ metabolism and reproduction. For example, when a CNS lymphoma is of B-cell origin, a monoclonal antibody targeting B-cells called Rituximab is often used.
- Corticosteroids: This class of medication is often used in the initial treatment for CNS lymphoma to help reduce swelling in the brain and temporarily reduce tumor size. While not a long-term treatment, corticosteroids can relieve inflammation and ease symptoms like headaches or other neurological issues.
- Antiretroviral therapy (ART): For patients with HIV and AIDS, treatment of the underlying HIV infection via antiretroviral therapy can help improve immune function and may reduce the risk or severity of CNS lymphoma. Patients with both CNS lymphoma and HIV or AIDS often receive a combination of ART and chemotherapy to treat both at the same time.
- Stem cell transplant: This nonsurgical procedure can be an option for patients who achieve remission via chemotherapy but have a high risk of relapse. Here, stem cells are harvested from your body and then undergo high-dose chemotherapy to destroy any remaining cancer cells. After chemotherapy, the harvested stem cells are reintroduced aid in bone marrow recovery and produce healthy blood cells. Because this is a more aggressive treatment, stem cell transplants are often done in younger lymphoma patients.
Radiation Therapy
Whole-brain radiation: When chemotherapy is ineffective, or if a person is too ill for chemotherapy, doctors can use whole-brain radiation to treat lymphomas of the central nervous system. Given the diffuse nature of CNS lymphoma, this is the most common type of radiation therapy given to patients with this condition.
Radiosurgery: While not considered surgery in a traditional sense, radiosurgery relies on precise radiation delivery systems to focus radiation at the tumor site—no cutting or stitching involved. Doctors often use this treatment for tumors that have come back, but rarely as initial treatment. Radiosurgery is infrequently used for CNS lymphoma. The two most common forms of radiosurgery are:
- Gamma Knife radiosurgery: This technique destroys malignant tissue through precisely focused radiation, meaning it’s only lethal to cells within the immediate vicinity. However, the Gamma Knife can only be used to treat lesions in the head, as it involves attaching a metal frame to the skull for complete accuracy.
- CyberKnife radiosurgery: This technique uses image-guided robotics to deliver surgically precise radiation to help destroy tumors like lymphoma while sparing healthy tissue.
Whole-brain radiation: When chemotherapy is ineffective, or if a person is too ill for chemotherapy, doctors can use whole-brain radiation to treat lymphomas of the central nervous system. Given the diffuse nature of CNS lymphoma, this is the most common type of radiation therapy given to patients with this condition.
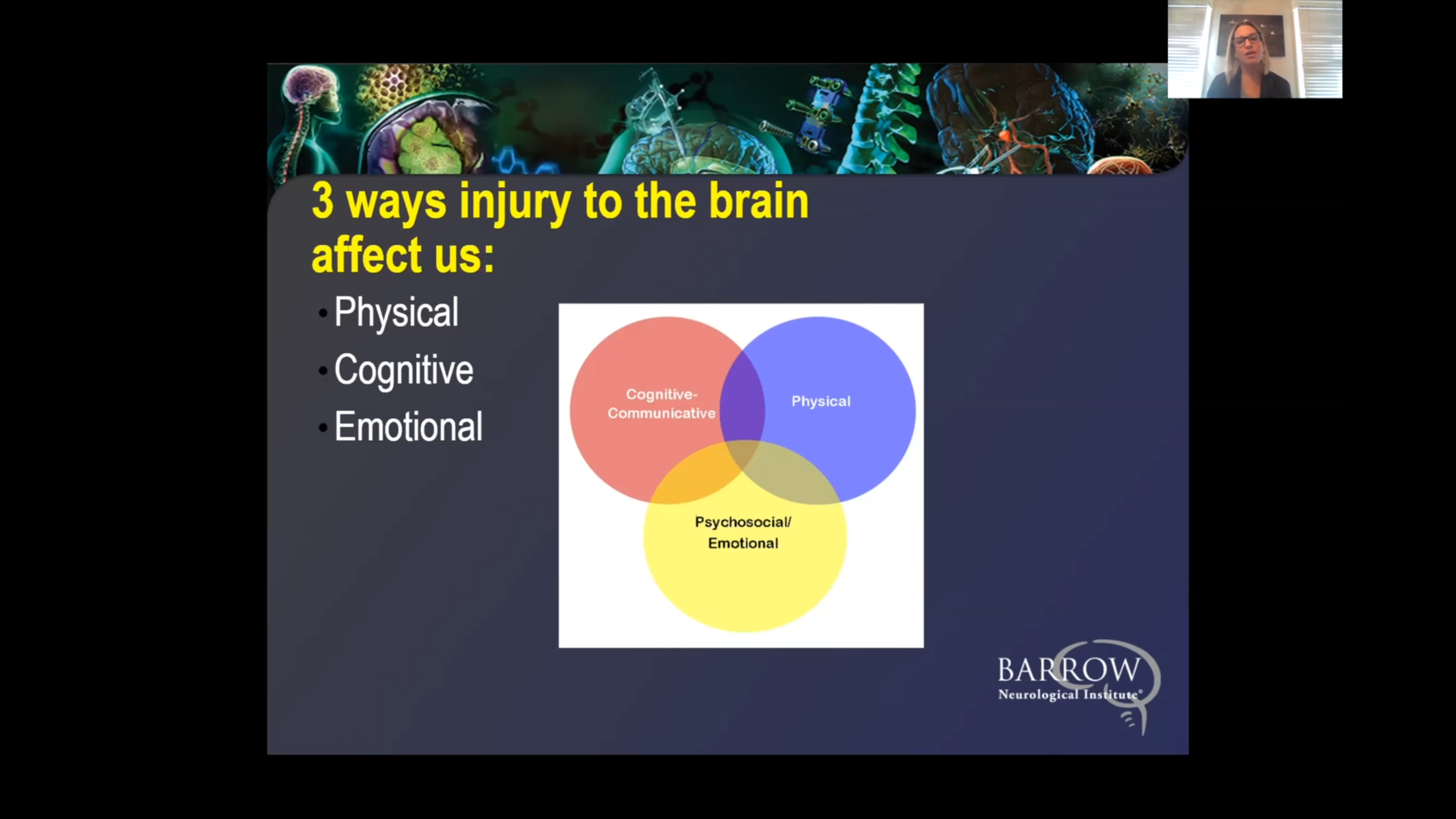
Sometimes, the symptoms of CNS lymphoma can improve dramatically after treatment. However, symptoms can also take a long time to improve because brain cells have a limited capability to regenerate. Sometimes, function can be regained by teaching other neurons to take over the job of damaged neurons using neuro-rehabilitation. Some people find their symptoms never completely disappear, although they improve over time.
One Central Location with Multiple Treatment Options
At Barrow Neurological Institute’s world-class Brain and Spine Tumor Program, we treat people with complex tumors like CNS lymphoma in one robust, full-service location. Our sophisticated multidisciplinary team—neurosurgeons, head and neck surgeons, neuro-oncologists, medical oncologists, and radiation oncologists, to name a few—can offer you the latest treatments for cancers affecting the nervous system, including metastatic cancers.
We also give our patients access to various neuro-rehabilitation specialists to maximize independence. Neuro-rehabilitation can include physical therapy to help you regain strength and balance, speech therapy to support speaking, expressing thoughts, or swallowing, and occupational therapy to aid you in managing daily activities like bathing, dressing, and using the bathroom. Treating a brain or spinal cord tumor is about more than extending your life—it’s also focused on enhancing your quality of life.
Clinical Trials
In partnership with the Ivy Brain Tumor Center, Barrow Neurological Institute is proud to be one of the country’s largest sites for neurological clinical trials.
Clinical trials are part of the cancer research process to determine if new treatments are safe, effective, or even better than the current standard treatment. Although not yet FDA-approved, clinical trials can be the best option for those with difficult-to-treat tumors to improve the odds of finding an effective treatment for them and for future patients. To search for clinical trials that are now enrolling, visit the Ivy Brain Tumor Center.
Common Questions
How common is CNS lymphoma?
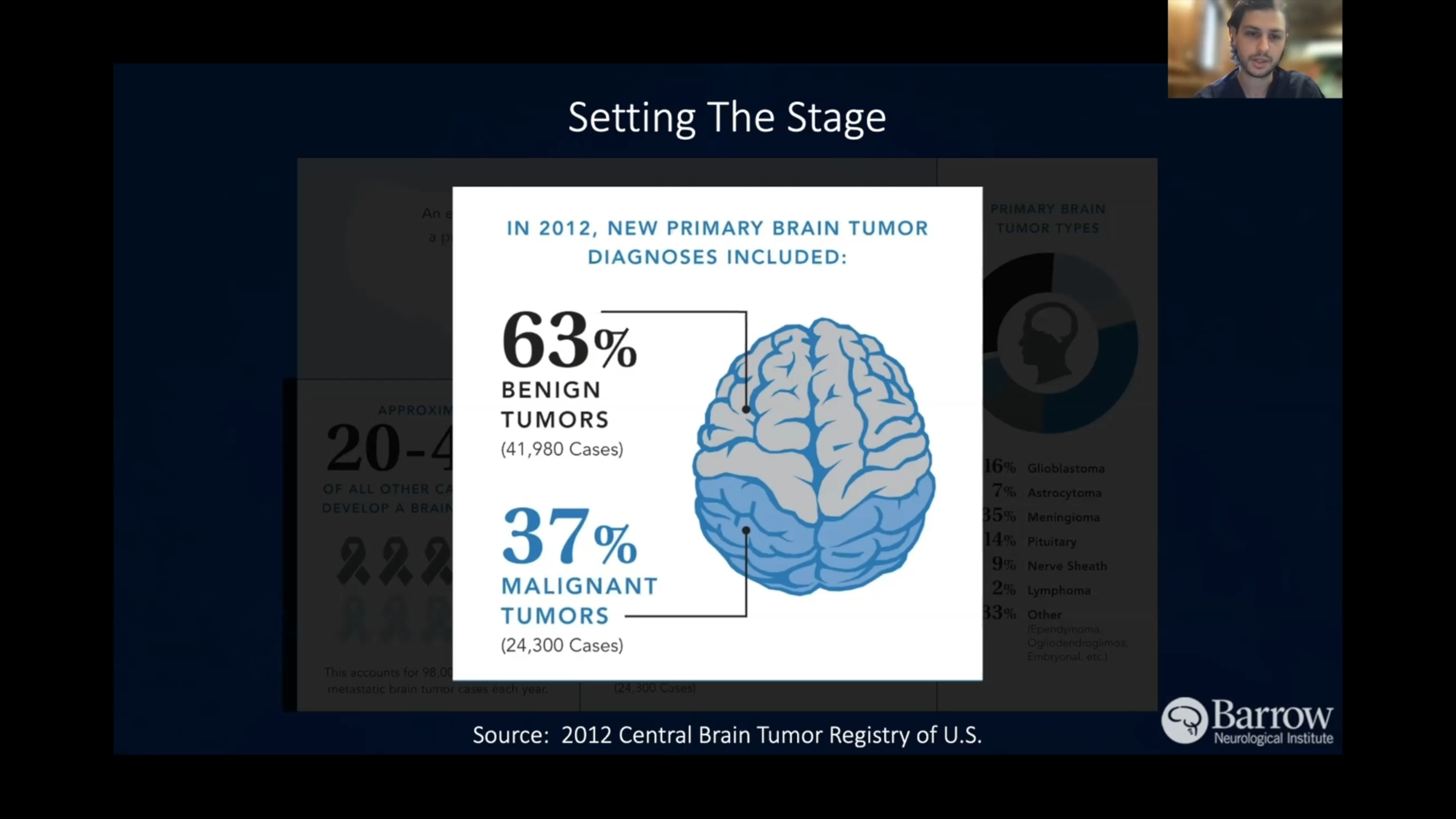
Central nervous system lymphoma (CNS lymphoma) accounts for one to two percent of all lymphomas and approximately two to three percent of all primary brain tumors.
The incidence of primary CNS lymphoma is estimated to be around 5 cases per 1,000,000 people each year. However, the risk is significantly higher in people with HIV or other immunosuppressive conditions.
Who gets CNS lymphoma?
Central nervous system lymphoma (CNS lymphoma) is more common in adults than children. Men are slightly more likely than women to develop the condition among adults.
Older adults—especially those over age 60—and individuals with weakened immune systems, like those with genetic immune deficiencies, people on long-term immunosuppressive therapy for autoimmune diseases, organ transplant recipients, and those diagnosed with HIV or AIDS are more likely to develop this rare form of non-Hodgkin’s lymphoma.
Although CNS lymphoma can appear in healthy individuals with no apparent risk factors, it remains significantly more common in those who have compromised immune systems.
What is the prognosis for those with CNS lymphoma?
The prognosis for central nervous system lymphoma (CNS lymphoma) can range from challenging to promising, depending on a person’s age, immune status, degree of lymphoma, and response to treatment. While CNS lymphoma is an aggressive cancer, some patients—particularly younger people with robust immune systems—can achieve remission and live full lives.
The five-year survival rate for primary CNS lymphoma is around thirty to fifty percent. However, this can be higher in younger patients who respond well to treatment. Those who achieve complete remission after the initial treatment have the best prognosis, with some individuals living many years or even being cured.
Unfortunately, CNS lymphoma has a high risk of relapse, especially in the first few years after treatment. That said, treatment advances like high-dose chemotherapy, stem cell transplants, and targeted therapies are improving overall outcomes.
Can CNS lymphoma be prevented?
Central nervous system lymphoma (CNS lymphoma) cannot be prevented entirely. However, certain steps can reduce your risk of developing CNS lymphoma, particularly if you’re at higher risk due to a weakened immune system. They include:
- Managing HIV and AIDS: Simply stated, people living with HIV are at a much higher risk of CNS lymphoma. This means that one of the most effective ways to lower this risk is by successfully managing HIV or AIDS through the appropriate therapies and medications.
- Avoid immunosuppression if possible: Organ transplant recipients and people with autoimmune diseases often need to take long-term immunosuppressive medications to prevent the rejection of transplanted organs. While immunosuppressive therapy is usually necessary, providers can carefully monitor patients for early signs of lymphoma and use the lowest effective dose of immunosuppressive drugs possible to manage the risk of CNS lymphoma.
- Limiting radiation exposure: Radiation exposure to the brain is a risk factor for numerous cancers, including lymphomas. If you’re undergoing radiation for another condition, your healthcare provider will carefully balance the need for radiation with the risk of developing secondary cancers like CNS lymphoma.
Maintaining a healthy lifestyle: Regular exercise, a balanced diet, and avoiding tobacco and excessive alcohol consumption reduce the risk of certain cancers.
Additional Resources
Brain Tumor Survivor & Caregiver Symposium
Neurosurgery
Neuro-Oncology
Radiation Oncology
Grit, Grace, and Brain Tumors: An Inside Outside Perspective
Clinical Trials
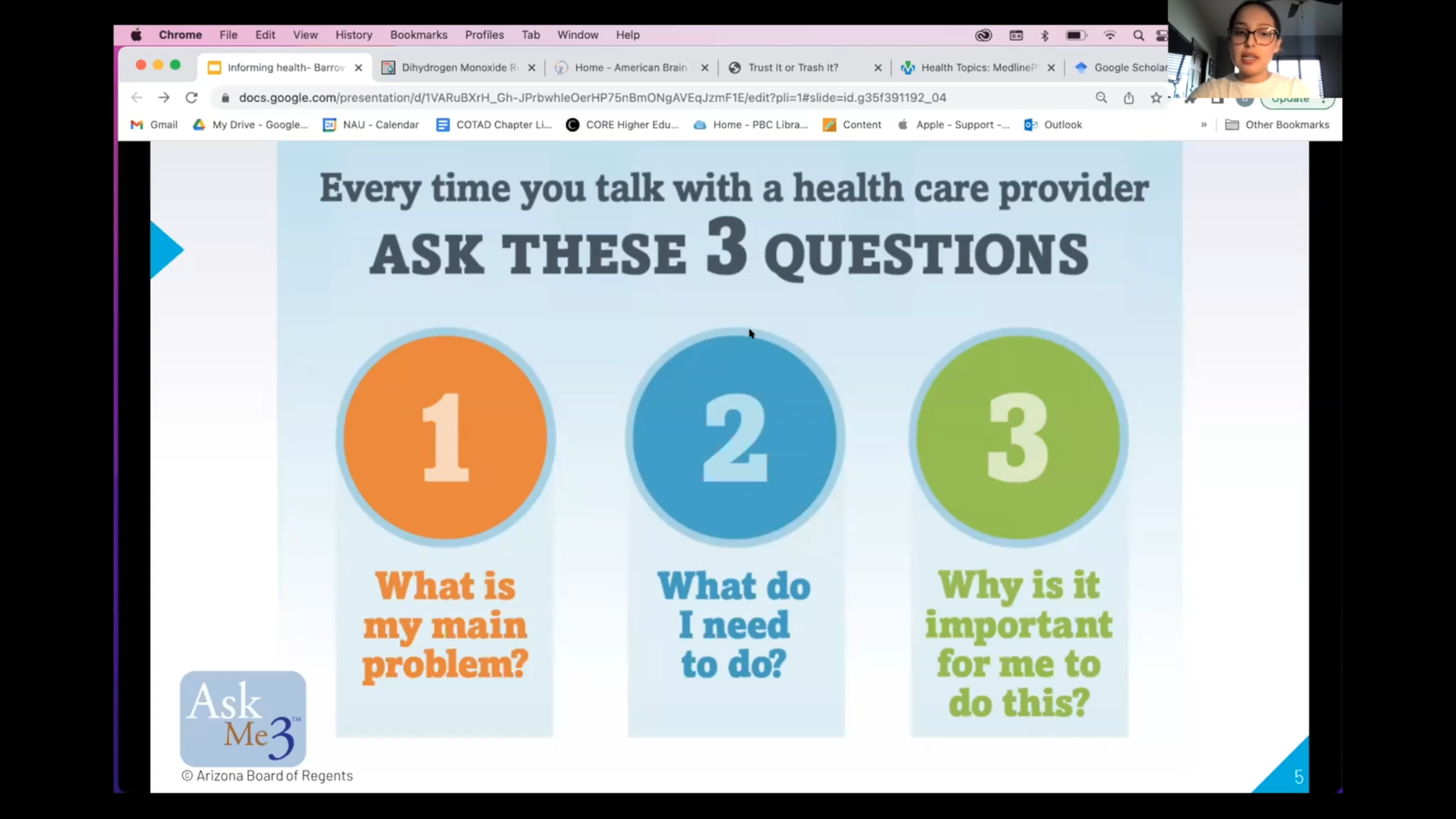
Informing Health: A Guide to Healthcare Information
Advancements in Brain Cancer Treatment

Trials to Triumph: Celebrating Every Victory in Brain Cancer Treatment
Discovering New Treatments For Brain Cancer

Revolutionizing Brain Tumor Treatment at the Ivy Brain Tumor Center
Brain Cancer Breakthrough: New Clinical Trial Tests Direct-to-Tumor Method



Request an Appointment
Call (602) 406-2800