
Odontoid Screw Fixation
Authors
Dimitris Konstantinou, MD †
Allan D.O. Levi, MD ‡
Volker K.H. Sonntag, MD
Curtis A. Dickman, MD
Division of Neurological Surgery, Barrow Neurological Institute, Mercy Healthcare Arizona, Phoenix, Arizona
Current Address:
†University Hospital of Patras, Patras, Greece
‡ University of Miami, Miami, Florida
Abstract
Thirty-two patients who sustained Type II fractures of the odontoid process were surgically treated with anterior odontoid screw fixation. Odontoid screw fixation is the preferred method for stabilization of acute, unstable Type II odontoid fractures. It is associated with excellent clinical results and a high rate of fusion. This is the only spinal fixation technique for fractures that restores spinal stability yet completely preserves normal spinal motion.
Key Words : atlantoaxial instability, cervical spine instability, odontoid fracture, odontoid screw fixation
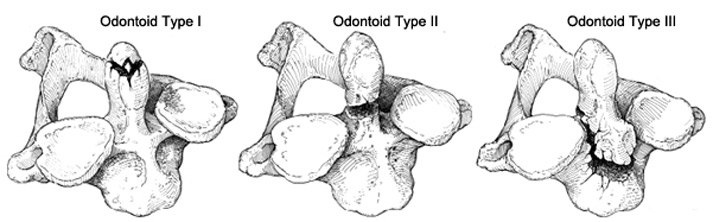
Almost two thirds of all dens fractures are Type II odontoid fractures or fractures that extend across the neck of the dens (Fig. 1).13Halo immobilization is the preferred treatment for fractures displaced less than 6 mm. Open surgical reduction and fixation are required for widely displaced fractures. Odontoid Type II fractures displaced more than 6 mm (anteriorly or posteriorly) have a 78% chance of failure when treated with a halo brace.13 When treatment is delayed more than 1 week, a patient is older than 60 years, the displacement is anterior, or all three conditions exist, these fractures have been associated with even higher rates of nonunion.3,9 Type IIA fractures (comminuted), an odontoid Type II fracture with bone fragments at the base of the odontoid, have a 100% failure rate when treated with a halo brace.17 The difficulty in obtaining union of a Type II odontoid fracture through halo immobilization has been attributed to disruption of the precarious blood supply of the odontoid process, free floating of the fractured odontoid bone in the surrounding synovial cavities, and limited contact between the two cancellous surfaces of the fracture.11
Surgical treatment for Type II odontoid fractures with posterior C1 C2 wiring methods is associated with a fusion rate of 97% but requires halo immobilization for 3 months after surgery and sacrifices all C1 C2 motion.2,8,10 C1 C2 posterior transarticular screws added to the wiring techniques eliminate the need for postoperative halo immobilization but also sacrifice normal rotation at this level. In contrast, anterior odontoid screw fixation provides immediate stability, preserves normal rotation at C1 C2, and usually obviates the need for halo immobilization after surgery. This article reviews our experience with anterior odontoid screw fixation for Type II odontoid fractures.
Materials and Methods
Between 1989 and 1996, 32 patients who sustained Type II fractures of the odontoid process underwent anterior odontoid screw fixation. There were 19 males and 13 females between 16 and 101 years old (mean, 41 years). The fractures were caused by a motor vehicle collision in 21 cases and by a fall in 11 cases. The time between injury and the operation ranged from 1 to 90 days (mean, 10 days).
All patients underwent a thorough radiologic evaluation (Fig. 2), including anteroposterior (AP) and lateral radiography, computed tomography (CT), and magnetic resonance imaging. The latter was performed to rule out a disruption of the transverse atlantal ligament.5 The mean AP displacement of the fracture was 8 mm (range, 4 to 13 mm). Five patients also had a C1 posterior arch fracture. Twenty seven patients were neurologically intact at the time of injury, and five patients presented with incomplete neurological lesions. All patients were initially treated with a halo brace or Philadelphia collar but had persistent instability or malalignment with a high risk of nonunion.

Fourteen patients sustained serious associated traumatic injuries. Six patients had severe head injuries, two had chest injuries, three had long bone fractures, one sustained intraabdominal injuries that required laparotomy, one had a pelvic fracture, and three had facial fractures.
Surgical Technique
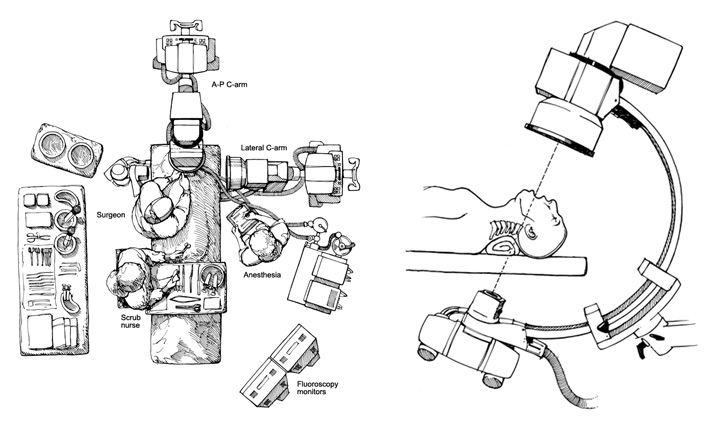
Intraoperative somatosensory evoked potential monitoring was performed in all patients to detect any changes during the procedure. General endotracheal anaesthesia was used and patients were placed in a supine position. The head was secured on a radiolucent operating table with the mouth held open with a radiolucent bite block so that AP and lateral fluoroscopy was available throughout the operation (Fig. 3). The patient’s head was positioned under lateral fluoroscopic guidance so that the neck could be extended to permit a trajectory for proper insertion of the screw (Fig. 4).
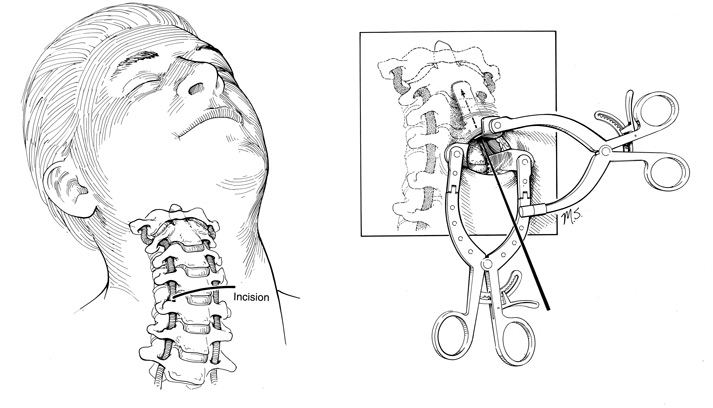
A transverse skin incision was made at the level of C5 C6. This incision was carried down through the platysma, which was widely undermined to allow optimal placement of the retractor. The anterior border of the sternocleidomastoid was identified, along with the carotid sheath, and mobilized laterally. The esophagus, trachea, and strap muscles were reflected medially. The anterior surface of the cervical spine was identified and the retropharyngeal space was opened to the level of C2. The medial borders of the longus colli muscles were coagulated and their bellies were elevated laterally. A transsphenoidal retractor was then introduced to retract the soft tissues laterally away from the spine.
The next goal was to identify the midline anteroinferior aspect of the body of C2. A midline gutter was cut into the anterior body of C3 and C2 C3 disk to provide adequate visualization of the anteroinferior end plate of C2. A drill guide was placed on the anteroinferior lip of C2 in the midline. Using the 2 mm bit on a pneumatic drill, real time biplanar fluoroscopy was used to monitor progress until the drill bit just penetrated the cortex of the odontoid tip. The drill bit was then backed out of the pilot hole, and a 2.7 mm tap was advanced under fluoroscopic control until it just penetrated the distal cortex of the dens. At this point, a partially threaded, nonself tapping, 3.5 or 4.0 mm diameter cancellous lag screw was selected. The screw was advanced under fluoroscopic control and tightened until the screw head was just countersunk with respect to the body of C2 and one or two threads of the screw penetrated through the tip of the dens. The wound was copiously irrigated and meticulous hemostasis was obtained before the platysma and skin were closed.
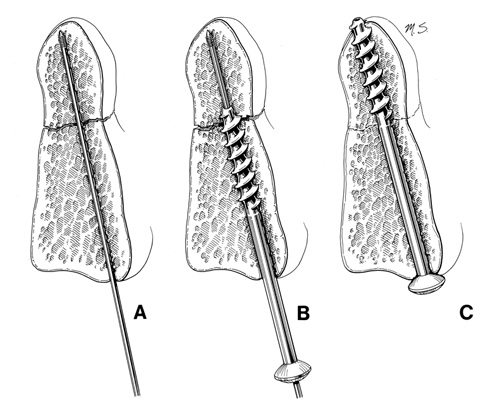
In 22 of the patients, a cannulated screw system was used to insert the screws (Fig. 5). Under fluoroscopic control, a 1.2 mm diameter Kirschner wire (K wire) was positioned on the anterior aspect of the inferior end plate of C2. The K wire was advanced with a pneumatic drill so that the tip engaged the cortex of the tip of the dens (Fig. 5A). After the K wire was positioned satisfactorily, the screw length was measured and a self tapping cannulated screw was inserted directly over the K wire until the tip of the screw engaged the tip of the dens (Fig. 5B). To achieve a lag effect, the screw threads did not cross the fracture line. After satisfactory placement of the screw, the K wire was removed (Fig. 5C).
Results
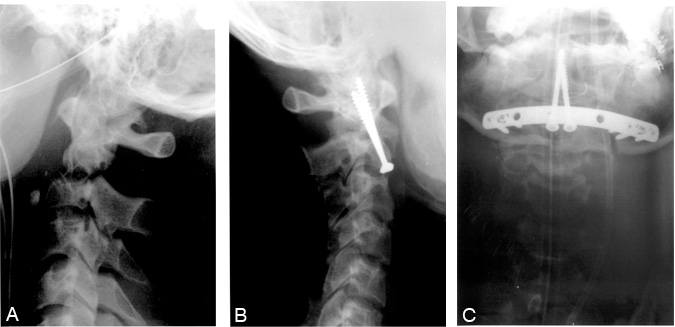
The indications for odontoid surgery were widely displaced odontoid fractures that could not be satisfactorily immobilized with an orthosis (n = 24) or patients who had failed halo immobilization (n = 8). The average screw length was 38 mm (range, 32 to 44 mm). Seven patients had bilateral odontoid screws placed (Fig. 6). Twenty five patients had one odontoid screw placed (Figs. 7 and 8). One patient who suffered from an odontoid Type II fracture and an unstable C1 burst fracture had one odontoid screw placed and also had bilateral anterior transarticular facet screws placed. Twenty seven patients wore a hard collar (Philadelphia or Miami) 3 months after surgery. Five patients with severe osteoporosis and extensive fractures remained in a halo brace for 3 months.
There were no intraoperative complications, and none of the 32 patients had postoperative neurological complications related to the odontoid screw fixation. Of the five patients who presented with a mild neurological deficit, three were normal at their follow up examination and two had improved. In one patient, a postoperative CT myelogram revealed that the screw (40 mm long) appeared to impinge on the subarachnoid space, and it was replaced with a 35 mm screw the next day without complications.
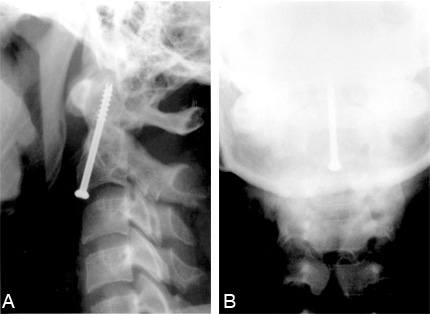

On follow up, 30 of the 32 patients had satisfactory healing of their fractures without nonunion, redisplacement, or hardware failure (91% fusion rate). Two patients had early failure of the screw within 2 weeks of surgery due to severe osteoporosis (Fig. 9). These two patients required posterior transarticular screw fixation and interspinous wiring. The postoperative flexion and extension radiographs of the 30 patients who underwent odontoid screw fixation demonstrated permanent cervical stability. At the follow-up clinical evaluation (median follow-up, 18 months), 27 of the 32 patients had full range of motion of the neck without pain. Five patients reported moderate restriction of neck motion. There was no difference in outcomes between cannulated and noncannulated odontoid screw fixation. None of the screws bent or broke.
Discussion
Anterior screw fixation of odontoid Type II fractures is associated with excellent clinical results and a 91% fusion rate in this series. This technique is unique because it completely preserves normal spinal motion, which is particularly prominent at the level of C1 C2. Half of all cervical rotation is sacrificed if C1 and C2 are fused.
Other reports in the literature concur with our findings on the results of odontoid screw fixation. Pointillart et al.15 reported 150 patients who were treated for odontoid Type II fractures. The rate of pseudarthrosis was 23% in patients treated nonoperatively with external orthoses, 20% in patients treated with posterior C1 C2 arthrodesis, and 5% in patients treated with anterior screw fixation. Montesano et al.14 treated 14 patients with an odontoid Type II fracture with anterior screw fixation. There were two cases of nonunion. Geisler et al.11 operated on nine patients with a Type II odontoid fracture. Immediately after surgery, two patients died, one from adult respiratory distress syndrome and cardiopulmonary arrest and the other from pulmonary hemorrhage during a bronchoscopic examination to clear copious pulmonary secretions. At follow-up, however, the surviving seven patients had excellent outcomes. Verheggen and Jansen18treated 18 patients with a Type II odontoid fracture with anterior screw fixation. One patient died after surgery from cardiopulmonary insufficiency. Two patients had to undergo revisions—one because the position of the screw was suboptimal and the other for nonunion of the dens 7 months after the first operation. Borne et al.4 treated nine patients for Type II odontoid fractures by odontoid screw fixation. In their series, they had no nonunions but two patients with severe preoperative tetraparesis died after surgery—one from infection and respiratory complications and one from cardiac failure.
Biomechanical studies of odontoid Type II fractures and screw fixation7,12,16 have found no statistically significant differences in the bending stiffness associated with one- and two-screw fixation in cadaveric specimens. In their load-to-failure experiments, Sasso et al.16 found that two screws were not significantly stronger than one screw. Although the two-screw technique may increase torsional stability, this finding may have limited clinical relevance. Overall, however, these data support the clinical use of one screw for odontoid fixation.
Odontoid screw fixation does not immediately restore normal strength to the dens. After screw fixation, the dens has only half of its original strength.16 Normal strength is not achieved until the fracture fully heals. Therefore, an orthosis should be used postoperatively to reduce the loads on the spine while the fracture heals. If the bone is severely osteoporotic, a halo brace may need to be used postoperatively.
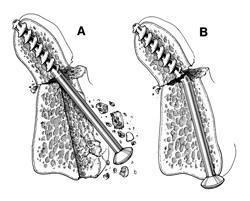
We use a lag screw that compresses the fractured bone surfaces together while they are held in anatomic alignment.6 The mechanical compression results from the force between the threads in the tip of the odontoid and the head of the screw on the cortex of the anteroinferior portion of the body of C2. The compression of the fractures improves the immobilization of the fragments and facilitates bone union.
In conclusion, anterior screw fixation of Type II odontoid fractures offers several advantages. It treats the fracture directly, has a high union rate, and preserves the normal rotational mobility of the atlantoaxial complex. Odontoid screw fixation is an excellent approach to the treatment of Type II odontoid fractures in patients with fractures dislocated more than 6 mm or in patients who cannot wear a halo orthosis.
References
- Anderson LD, D’Alonzo RT: Fractures of the odontoid process of the axis. J Bone Joint Surg (Am) 56:1663-1674, 1974
- Apfelbaum RI: Anterior screw fixation of odontoid fractures, in Camins MD, O’Leary PF (eds): Diseases of the Cervical Spine. Baltimore: Williams & Wilkins, 1992, pp 603 608
- Apuzzo MLJ, Heiden JS, Weiss MH, et al: Acute fractures of the odontoid process. An analysis of 45 cases. J Neurosurg 48:85 91, 1978
- Borne GM, Bedou GL, Pinaudeau M, et al: Odontoid process fracture osteosynthesis with a direct screw fixation technique in nine consecutive cases. J Neurosurg 68:223 226, 1988
- Dickman CA, Mamourian A, Sonntag VKH, et al: Magnetic resonance imaging of the transverse atlantal ligament for the evaluation of atlantoaxial instability. J Neurosurg 75:221 227, 1991
- Dickman CA, Sonntag VKH, Marcotte PJ: Techniques of screw fixation of the cervical spine. BNI Quarterly 8:9 26, 1992
- Doherty BJ, Heggeness MH, Esses SI: A biomechanical study of odontoid fractures and fracture fixation. Spine 18:178 184, 1993
- Duncan RW, Esses SI: Dens fractures: Specifications and management. Semin Spine Surg 18:19 27, 1996
- Dunn ME, Seljeskog EL: Experience in the management of odontoid process injuries: An analysis of 128 cases. Neurosurgery 18:306 310, 1986
- Fried LC: Atlanto axial fracture dislocations. Failure of posterior C1 to C2 fusion. J Bone Joint Surg 55:490 496, 1973
- Geisler FH, Cheng C, Poka A, et al: Anterior screw fixation of posteriorly displaced type II odontoid fractures. Neurosurgery 25:30 38, 1989
- Graziano G, Jaggers C, Lee M, et al: A comparative study of fixation techniques for type II fractures of the odontoid process. Spine 18:2383 2387, 1993
- Hadley MN, Dickman CA, Browner CM, et al: Acute axis fractures: A review of 229 cases. J Neurosurg 71:642 647, 1989
- Montesano PX, Anderson PA, Schlehr F, et al: Odontoid fractures treated by anterior odontoid screw fixation. Spine 16:33 37, 1991
- Pointillart V, Orta AL, Freitas J, et al: Odontoid fractures. Review of 150 cases and practical application for treatment. Eur Spine J 3:282 285, 1994
- Sasso R, Doherty BJ, Crawford MJ, et al: Biomechanics of odontoid fracture fixation. Comparison of the one and two screw technique. Spine 18:1950 1953, 1993
- Sonntag VKH, Dickman CA, Vardiman A: Anterior odontoid screw fixation, in Menezes AH, Sonntag VKH (eds): Principles of Spinal Surgery. New York: McGraw Hill, 1996, pp 1039 1949
- Verheggen R, Jansen J: Fractures of the odontoid process: Analysis of the functional results after surgery. Eur Spine J 3:146 150, 1994