
Posterior Screw-Plate Fixation of the Cervicothoracic Junction with Cervical Lateral Mass and Thoracic Transverse Process Screws: Case Report
Authors
Mark Gerber, MD
Curtis A. Dickman, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
Posterior fixation of the cervicothoracic junction can be technically challenging. We present a patient with C6-C7 locked facets that were reduced posteriorly and fixated using plates anchored with lateral mass screws at C6 and with transverse process screws at T1.
Key Words: locked facets, transverse process screw
Due to the unfavorable anatomy of C7, placement of lateral mass or pedicle screws at this level can be risky even with image guidance. Placement of thoracic pedicle screws can also be difficult. The transverse processes of T1 may provide a safe and useful alternative point of fixation when constructs are required to span the cervicothoracic junction.
Illustrative Case
A 50-year-old female was the restrained driver of a vehicle involved in a rollover accident. The patient briefly lost consciousness and complained of numbness in her arms and legs in addition to an inability to move her legs.
She was brought to our facility as a trauma victim and was resuscitated according to the advanced trauma life support (ATLS) protocol. Plain radiographs of the cervical spine raised concern about bilateral locked facets at C6-7. A complete neurological examination showed that the patient had a complete spinal cord injury with 3/5 strength in the triceps. C7 was the last level of function. There was no detectable preservation of sensory function below the level of injury.
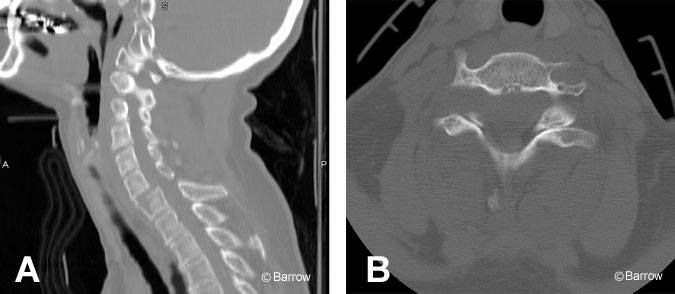
A halo ring was attached to the patient’s head after a basic head computed tomography (CT) showed no intracranial pathology. CT of the cervical spine also was obtained to confirm the suspicion of locked cervical facets (Fig. 1). Closed reduction was attempted without success. Magnetic resonance (MR) imaging was attempted, but significant artifact impaired visualization. The patient was placed in cervical traction after closed reduction failed.
Within 24 hours of injury, the patient underwent a posterior approach for open reduction and internal fixation of the locked facets. The superior articulating facets of C7 required drilling to achieve reduction. A single titanium Songer cable was used for C6-C7 spinous process wiring.
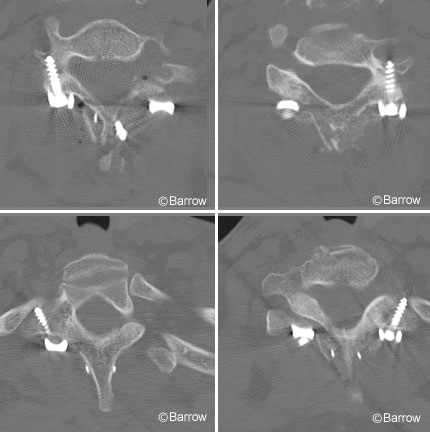
A novel technique was used for posterior cervical plating. Lateral mass screws were used to anchor the superior end of the lateral mass plates at C6 (Fig. 2). Then 14-mm long, 4.0-mm diameter bone screws were advanced into the transverse process of T1 to achieve fixation inferiorly. Iliac crest bone graft was placed over the roughened surfaces of the spinous processes, lamina, and facet joints of C6 through T1. Postoperative CT confirmed that the screws were well placed with bicortical purchase of the transverse processes. The patient wore a halo vest after surgery and regained significant function of her lower extremities by postoperative Day 4. At follow up 4 months after surgery, she had recovered the ability to ambulate independently and to use her arms fully. She had a well-formed bone fusion on postoperative radiographs.
Discussion
The surgical treatment of locked facets is controversial.[2,3] Early reduction of locked facets is a primary consideration regardless of the technique used. In our patient, a novel approach was used to secure the lateral mass plate at the cervicothoracic junction. The bilateral locked facets were reduced from a posterior approach, and lateral mass plates were then used to further strengthen the construct.
Pedicle screw fixation may have been an alternative treatment, but the difficulties associated with placing lower cervical and thoracic pedicle screws are well known. Image guidance is a significant aid to the placement of instrumentation at these levels. However, issues with image guidance, such as registration of the navigation system to mobile bony landmarks, can be problematic.
In a biomechanical analysis performed by Heller et al.,[1] transverse process screws at T1 were found to sustain a similar load to failure as pedicle screws placed at this level. Below T1, transverse process screws were unable to tolerate the same load as pedicle screws. Our case illustrates that the placement of transverse process screws at T1 may provide a less technically demanding, yet safe and structurally sound alternative to pedicle screw fixation when short segment fusion through the cervicothoracic junction is required.
References
- Heller JG, Shuster JK, Hutton WC: Pedicle and transverse process screws of the upper thoracic spine: Biomechanical comparison of loads to failure. Spine 24:654-658, 1999
- Jones EL, Heller JG, Silcox DH, et al: Cervical pedicle screws versus lateral mass screws. Anatomic feasibility and biomechanical comparison. Spine 22:977-982, 1997
- Wolf A, Levi L, Mirvis S, et al: Operative management of bilateral facet dislocation. J Neurosurg 75:883-890, 1991