
Pineal Region Germinoma in the Seventh Decade: Case Report
Authors
Jeffrey D. Klopfenstein, MD
Giuseppe Lanzino, MD*
Louis J. Kim, MD
Robert F. Spetzler, MD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
*Current Address: Department of Neurosurgery, University of Illinois College of Medicine at Peoria, Peoria, Illinois
Abstract
Intracranial germinomas are typically considered tumors of children and young adults, but they can occur in older adults. A 61-year-old male presented with confusion, gait difficulties, and visual disturbances. Magnetic resonance imaging revealed a 3 x 2 x 2 cm, heterogeneously enhancing mass in the pineal region causing obstructive hydrocephalus. The patient underwent ventriculoperitoneal shunting at an outside institution and was transferred to our facility for definitive treatment of the tumor. The patient underwent an occipital craniotomy and a supracerebellar infratentorial approach for resection of his pineal region tumor. Histopathologic examination revealed characteristics classic for germinoma, and the patient was referred for radiation therapy. Only four patients older than 60 years have been reported with a confirmed intracranial germinoma. Our case further underlines that intracranial germinomas can occur in older adults. Because radiation therapy is curative for these tumors, surgeons must recognize the potential for germinoma in older patients to avoid unnecessary and potentially harmful radical resection.
Key Words: age, germinoma, pineal region
Germinomas are rare neoplasms of the central nervous system and account for 0.2 to 1.7% of all primary intracranial tumors.[16] Most of these tumors occur in children and young adults; the mean age of onset is about 17 years.[5,12,18,23] Four cases of histopathologically confirmed intracranial germinoma in patients older than age 60 have been published.[2,5,10,11] We present the fifth such patient. The primary clinical relevance of this topic is the treatment of patients with this condition. Because radiotherapy is curative for germinoma, neurosurgeons must recognize that, although rare, this tumor can occur in older adults and need not be radically resected.
Illustrative Case
A 61-year-old man sought treatment at an outside facility after 5 weeks of worsening confusion, emotional lability, ataxia, and visual difficulties. Initial imaging studies showed a pineal region mass with obstructive hydrocephalus. A ventriculoperitoneal (VP) shunt was placed to treat the patient’s hydrocephalus, and he was referred to our institution for definitive treatment of the pineal region mass.
The patient’s general examination was unremarkable and his neurological examination was significant only for an unsteady gait. The surgical incisions from placement of the VP shunt had healed well.
{kind=link}
Diagnostic Imaging
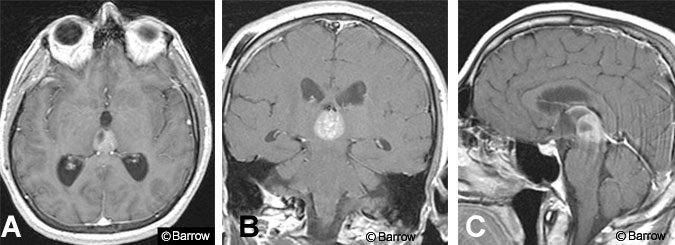
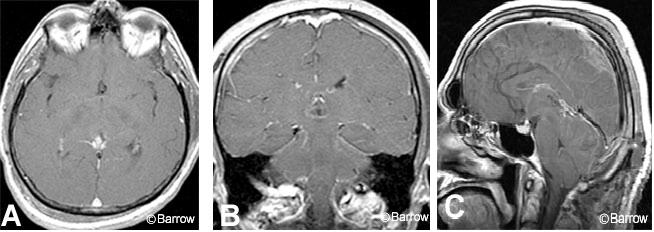
Magnetic resonance (MR) imaging of the brain with and without gadolinium showed a 3 x 2 x 2 cm, heterogeneously enhancing mass in the third ventricle just anterior to the pineal gland (Fig.1). Mild ventriculomegaly persisted. The imaging characteristics were considered consistent with pineocytoma. Other lesions included in the differential diagnosis were pineoblastoma, glioma, central neurocytoma, and metastases. Given the patient’s age, intracranial germ cell tumors, including germinomas, were considered to be highly unlikely.
Intervention
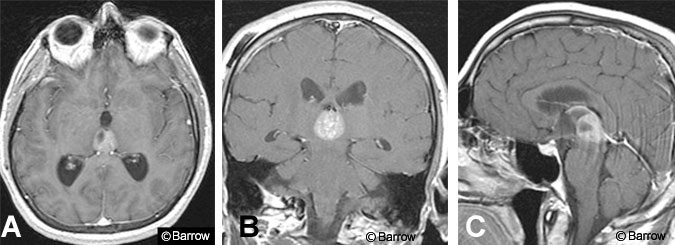
An occipital craniotomy was performed followed by an image-guided supracerebellar infratentorial approach to the pineal region (Fig. 2). Immediately apparent was a large mass arising directly from the posterior third ventricle. The tumor was tan and soft and there was no obvious capsule. Gross total resection was performed and multiple specimens were sent for histopathologic analysis. Closure was routine, and the patient was transferred to the recovery room in stable condition.
Histopathologic Examination
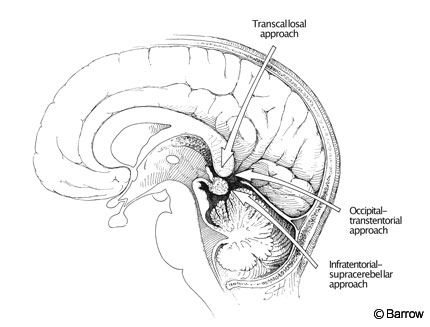
Intraoperative frozen sections were interpreted as a non-small cell neoplasm consistent with marked lymphocytic reaction favoring germinoma. Microscopic examination of permanent sections revealed sheets of neoplastic cells with large rounded nuclei and a moderate amount of eosinophilic cytoplasm (Fig. 3). Aggregates of lymphocytes were scattered among the neoplastic cells, particularly in adjacent fibrovascular connective tissues. Special staining revealed positivity for placental alkaline phosphatase and glycogen. Based on these findings, the final pathologic diagnosis was germinoma.
Postoperative Course
On the first postoperative day, the patient was somnolent and confused. MR imaging revealed gross total resection of the tumor but also an occipital epidural hematoma, which was evacuated without difficulty. Thereafter, the patient convalesced uneventfully and his neurologic function improved steadily. Radiotherapy was arranged after consulting with radiation oncology and neurooncology.
At discharge, the patient was awake, fully oriented, and able to mobilize with minimal difficulty. Neurological deficits included mild ataxia, upgaze palsy, nystagmus, and moderate swallowing difficulties requiring percutaneous endoscopic gastrostomy (PEG). At his 6-week follow-up examination, the patient had improved significantly and his dysphagia had resolved enough to discontinue the PEG.
Postoperative MR imaging of the entire neuraxis confirmed gross total resection of the pineal region mass with no evidence of seeding (Fig. 4). Levels of serum markers, including human chorionic gonadotropin and alpha fetoprotein, were within normal limits ruling out a mixed intracranial germ cell tumor.
Discussion
Intracranial germ cell tumors account for 0.3% to 3.4% of all primary brain tumors in Western countries.[7,9,10,14,24] In Japan the incidence in- creases to between 4.8% and 15%.[13,17,22] Germinomas are the most common, composing 36 to 65% of all germ cell tumors.[2,10,12,18,20] In the United States, the estimated incidence of intracranial germinoma is 0.1/100,000 population.[8]
Intracranial germinomas typically occur in the suprasellar region (49%), followed by the pineal region (38%), both pineal and suprasellar regions (8%), and other locations (5%).10 Spinal cord metastases have been reported in 10 to 20% of patients.[3,4,9,19] Males are most often affected by intracranial germinoma by a ratio of 1.88:1. Unlike many of their germ cell tumor counterparts, germinomas do not consistently elevate serum levels of human chorionic gonadotropin or alpha fetoprotein.
The mean age of patients with intracranial germinoma at presentation is between 16 and 18 years; 84% become symptomatic between the ages of 9 and 27 years.[5,10,12] Less than 5% present after the age of 27 years. The youngest reported case is a 16-month-old boy[1] while the oldest is an adult between 70 and 80 years old (the patient’s exact age and sex were not provided).[2]
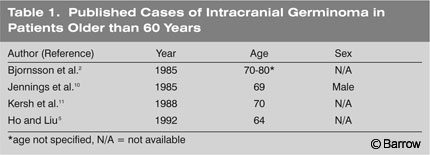
The English language literature contains four other reports of histologically confirmed intracranial germinoma in patients older than 60 years (Table 1).[2,5,10,11] Two patients were in their eighth decade and two were in their seventh. All had histologically confirmed intracranial germinoma. Because the four patients were included as members of series, details about sex, location, management, and outcomes were unavailable.
Despite the rarity of germinomas in older adults, it is imperative that they be included in the differential diagnosis of patients with a pineal or suprasellar mass to ensure their appropriate management. Management strategies for intracranial germinoma vary and are somewhat controversial.[6,9,11,12,15,20,21,23] However, the tumor’s exquisite sensitivity to radiation therapy is undisputed.[12,20] This radiosensitivity significantly reduces the need for radical resection of histologically confirmed germinoma and the potential morbidity associated with such a resection, particularly in older patients.
In conclusion, germinomas can and do occur in older adults. Surgeons must be aware of this possibility because management of these lesions requires less aggressive resection than other tumors common to elderly patients. Once the initial histopathologic diagnosis is established as germinoma, debulking should proceed only as needed to avoid undue risk to the patient. Long-term control of the lesion is ultimately achieved via radiation therapy.
References
- Ammar A, al-Majid H, Kutty MK: Germinoma in a 16-month old baby: A case report with brief review of the literature. Acta Neurochir (Wien) 110:189-192, 1991
- Bjornsson J, Scheithauer BW, Okazaki H, et al: Intracranial germ cell tumors: Pathobiological and immunohistochemical aspects of 70 cases. J Neuropathol Exp Neurol 44:32-46, 1985
- Chapman PH, Linggood RM: The management of pineal area tumors: A recent reappraisal. Cancer 46 :1253-1257, 1980
- Handa H, Yamashita J: Current treatment of pineal tumors (author’s transl) (Japanese). Neurol Med Chir (Tokyo) 21:147-154, 1981
- Ho DM, Liu HC: Primary intracranial germ cell tumor. Pathologic study of 51 patients. Cancer 70:1577-1584, 1992
- Hoffman HJ, Otsubo H, Hendrick EB, et al: Intracranial germ-cell tumors in children. J Neurosurg 74:545-551, 1991
- Hoffman HJ, Yoshida M, Becker LE, et al: Experience with pineal region tumours in childhood. Neurol Res 6:107-112, 1984
- Horowitz MB, Hall WA: Central nervous system germinomas. A review. Arch Neurol 48:652-657, 1991
- Jenkin RD, Simpson WJ, Keen CW: Pineal and suprasellar germinomas. Results of radiation treatment. J Neurosurg 48:99-107, 1978
- Jennings MT, Gelman R, Hochberg F: Intracranial germ-cell tumors: Natural history and pathogenesis. J Neurosurg 63:155-167, 1985
- Kersh CR, Constable WC, Eisert DR, et al: Primary central nervous system germ cell tumors. Effect of histologic confirmation on radiotherapy. Cancer 61:2148-2152, 1988
- Matsutani M, Sano K, Takakura K, et al: Primary intracranial germ cell tumors: A clinical analysis of 153 histologically verified cases. J Neurosurg 86:446-455, 1997
- Matsutani M, Takakura K, Sano K: Primary intracranial germ cell tumors: Pathology and treatment. Prog Exp Tumor Res 30:307-312, 1987
- Nishiyama RH, Batsakis JG, Weaver DK, et al: Germinal neoplasms of the central nervous system. Arch Surg 93:342-347, 1966
- Pertuiset B, Visot A, Metzger J: Diagnosis of pinealoblastomas by positive response to cobalt-therapy. Acta Neurochir (Wien) 34: 151-152, 1976
- Rosenblum MD, Matsutani M, Van Meir EG: CNS germ cell tumors, in Kleinhues P, Cavenee WK (eds): World Health Organization Classification of Tumours, Pathology and Genetics, Tumours of the Nervous System. IARC Press, 2000, pp 207-214
- Sano K: Pinealoma in children. Childs Brain 2:67-72, 1976
- Sano K: Pathogenesis of intracranial germ cell tumors reconsidered. J Neurosurg 90:258-264, 1999
- Sano K, Matsutani M: Pinealoma (germinoma) treated by direct surgery and postoperative irradiation. A long-term follow-up. Childs Brain 8:81-97, 1981
- Schild SE, Scheithauer BW, Haddock MG, et al: Histologically confirmed pineal tumors and other germ cell tumors of the brain. Cancer 78:2564-2571, 1996
- Spiegel AM, Di Chiro G, Gorden P, et al: Diagnosis of radiosensitive hypothalamic tumors without craniotomy: Endocrine and neuroradiologic studies of intracranial atypical teratomas. Ann Intern Med 85:290-293, 1976
- Takakura K: Intracranial germ cell tumors. Clin Neurosurg 32:429-444, 1985
- Vaquero J, Ramiro J, Martinez R, et al: Neurosurgical experience with tumours of the pineal region at Clinica Puerta de Hierro. Acta Neurochir (Wien) 116:23-32, 1992
- Wara WM, Jenkin RD, Evans A, et al: Tumors of the pineal and suprasellar region: Childrens Cancer Study Group treatment results 1960-1975: A report from Childrens Cancer Study Group. Cancer 43:698-701, 1979