
Reliability and Validity Studies for the German Adaptation of the BNI Screen for Higher Cerebral Functions
Author
Ramin Momtazi, MS
Neurological Rehabilitation Clinic Hilchenbach, Department of Clinical Neuropsychology, Hilchenbach, Germany
Abstract
The speech and language, memory, and orientation items of the BNI Screen (BNIS) for Higher Cerebral Functions were translated into German so that the entire test could be administered to German-speaking individuals. The spontaneous affect item was also altered because of cultural differences in the appreciation of symbolic meaning. To measure test-retest reliability, the German adaptation of the BNIS was administered to 20 brain dysfunctional individuals twice by different administrators. The correlation of the BNIS Total score between the two administrations was +.894. The correlation between the BNIS Total score and the total score of the Mini-Mental State examination (MMSE) was .817. These findings replicate observations obtained in a standardization study of the BNIS using an English-speaking, American population. Forty nonbrain-injured, German-speaking individuals also were administered the BNIS. Their scores were reliably higher than those of the patients. The German adaptation of the BNIS appears to be a reliable and valid neuropsychological screening test for the German population.
Key Words: BNI Screen, higher cerebral functions, neuropsychology, psychological testing
The BNI Screen (BNIS) for Higher Cerebral Functions is a brief neuropsychological screening instrument that provides both qualitative and quantitative information. Its seven subtests measure speech and language, visuospatial and visual problem solving, affect perception and expression, awareness, orientation, attention-concentration, and memory. Its inter-rater reliability and test-retest reliability are good.[6] Its construct validity in relationship to other screening instruments is also good, and its subtests appear to discriminate right and left hemispheric dysfunction in some patients.[6] The Total score on the BNIS provides a good estimate of sensitivity.[3] The summary information from this brief screening instrument correlates significantly with well-established, more extensive neuropsychological tests.[4] There is evidence that the BNIS may be useful in the clinical assessment of patients with dementia of the Alzheimer’s type.[5]
To be able to administer the BNIS to a German-speaking population, it was necessary to translate the speech and language, orientation, and memory subtests into German. Because of cultural differences, the spontaneous affect subtest was also altered. Changing these items in the German version necessitated evaluation of its reliability and validity. All other subtests are identical to the original version. The present study examined the inter-rater reliability and the concurrent and construct validity of the German version of the BNIS.
Materials and Methods
Subjects
Twenty brain dysfunctional patients (10 males, 10 females; mean age, 46.75; standard deviation (SD)=14.03) and 40 healthy controls (14 males, 26 females; mean age, 39.95 years; SD=14.67) were examined. The former had documented brain disorders and had been referred to our Department of Clinical Neuropsychology for neuropsychological examination. These nonbrain-damaged individuals were recruited from acquaintances and a general medical practice. Individuals with a history of neurological or psychiatric illness were excluded. The mean ages of the two groups were not significantly different (t =–1.72; p> .05). There was also no significant difference in years of education. The mean chronicity (i.e., time since onset) of the brain dysfunctional patients was 90.9 days (SD=67.7; range 20 to 250 days). In these patients the most common diagnosis was cerebrovascular accident (n=14). The remaining six patients had a traumatic brain injury.

Procedures
The German version of the BNIS is similar to the original version and also consists of a laminated stimulus booklet and a record form that has been translated into German. The items of the subscale speech and language and delayed recall were translated with consideration given to the linguistic properties of the contents. The orientation item was translated directly into German. The spontaneous affect item was altered to account for cultural differences in the appreciation of symbolic meanings (Fig. 1). The administration of the German version of the BNIS is identical to that of the original version, which is described elsewhere.[2,3] The general instructions for administration as well as the scoring instructions for specific items were translated into German to ensure objectivity and standardized administration.
In this study the German adaptation of the BNIS was administered by an experienced clinical neuropsychologist and by a graduate student of psychology who was trained and instructed in the principles of psychological testing and administration of the BNIS.
The BNIS was administered once to the normal controls. The BNIS was administered twice to the brain dysfunctional patients by two different examiners separately within 3 to 7 days. The correlation between the test and retest provided a measure of test-retest reliability. Because the BNIS was administered by two different examiners, its inter-rater reliability was also assessed. An official German version of the Mini-Mental State Examination (MMSE)[1] was administered to the patients to obtain a measure of construct validity.
Data Analysis
All statistical analyses were performed using the Statistical Program for Social Sciences-10 for Windows. Descriptive statistics were calculated for both groups. Age and education in both groups were compared by t-tests. Pearson correlation coefficients were calculated for the subscale scores, for the Total scores, for the two administrations of the BNIS, and for the Total scores of the BNIS and MMSE in the brain dysfunctional patients. The Total scores of the normal controls and the neurological patients on the BNIS were compared by a Mann-Whitney U-Test.
Results
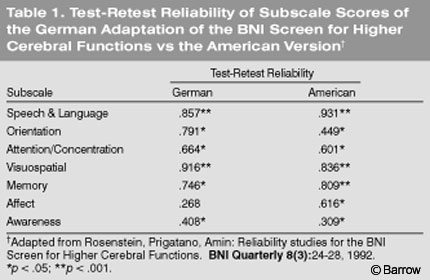
The test-retest reliability of the German adaptation of the BNIS in the brain dysfunctional patients, as calculated by the correlation between the two administrations by different examiners, was statistically significant for the total score (r =.894; p<.001). This finding replicates observations from an English-speaking American population.[6] The test-retest reliability coefficients for each subtest of the BNIS ranged from .268 to .916. The correlations for test-retest reliability were strikingly similar between German speaking individuals and those given the test in the initial American standardization studies (Table 1).
The correlation between the BNI Total score from the first administration and the MMSE Total score in the brain dysfunctional patients was .817 (p<.001). The shared common variance was 66.7 %. This finding also replicates the findings obtained when the BNIS was validated in an American study.[2] Prigatano[2] reported a correlation of .71 between the MMSE and the BNIS Total score. This measure of current validity was therefore also replicated.
The German patients’ Total score was significantly lower than that of the German control group as shown by a Mann-Whitney U-Test (z=–5.73; p<.001). The mean score of brain dysfunctional patients was 35 (SD=6.7; range, 26 to 48), and the mean score of the normal control subjects was 47 (SD=2.4; range, 41 to 50). Using a cut-off score of 47 to identify brain dysfunctional patients, the BNIS Total score had a sensitivity value of 90% and a specificity value of 77.5%. These findings are also consistent with the observations obtained in an American standardization study.[3]
Discussion
German-speaking countries have a great need for reliable and valid screening tests that provide both quantitative and qualitative information about the neuropsychological strengths and weaknesses of patients. Despite the importance of such instruments, appropriate measures for assessing both cognitive and affective disturbances in a neurological population are lacking.
This initial validity and reliability study replicates what has been observed in American populations. Both the test-retest reliability of the instrument and its concurrent validity are strikingly similar to observations by Prigatano[2] and Rosenstein, Prigatano, and Amin.[6] Thus, modification of the language items and affect item on the BNIS for a German-speaking group resulted in correlations similar to those obtained in the American population.
This study should be replicated with a larger group of German-speaking brain dysfunctional patients and normal controls. However, the initial findings are encouraging and suggest that the German version of the BNIS may be used to evaluate German-speaking individuals. Future studies should specifically consider expanding the sample size and evaluating whether the BNIS shows ecological validity of the type reported by Wass et al.[7] (See An Analysis of the Construct-Related and Ecological Validity of the BNI Screen for Higher Cerebral Functions: A Synopsis in this issue.)
Conclusion
The German adaptation of the BNIS seems to be promising for screening patients for cognitive and affective deficits associated with brain damage. This study found that the test-retest reliability and construct validity of the BNIS were satisfactory and comparable to findings in the American population on which the test was initially standardized.
Acknowledgments
The present study was performed in the course of a master’s thesis by Henning Schmitz-Peiffer. The data were collected in the Clinic Bavaria Kreischa in Kreischa, Germany. The author recognizes Frank Ostermann for his support in translating the speech and language items into German.
References
- Kessler J, Markowitsch HJ, Denzler PE: Mini-Mental State. MMST. Belz: Weinheim, 1990
- Prigatano GP: BNI Screen for Higher Cerebral Functions: Rationale and initial validation. BNI Quarterly 7(1):2-9, 1991
- Prigatano GP, Amin K, Rosenstein LD: Manual for the BNI Screen for Higher Cerebral Functions. Phoenix: Barrow Neurological Institute, 1995
- Prigatano GP, Palencia B: Halstead Impairment Index, Wechsler IQ, and the BNI Screen for Higher Cerebral Functions. BNI Quarterly 16(3):22-27, 2000
- Prigatano GP, Smason I: Assessment of Alzheimer’s patients with the BNI Screen for Higher Cerebral Functions. BNI Quarterly 10(2):30-35, 1994
- Rosenstein LD, Prigatano GP, Amin K: Reliability studies for the BNI Screen for Higher Cerebral Functions. BNI Quarterly 8(3):24-28, 1992
- Wass PJ: An Analysis of the Construct-Related and Ecological Validity of the Barrow Neurological Institute Screen for Higher Cerebral Functions (dissertation). Windsor, Ontario, Canada: University of Windsor, 1997