
Test-Retest Reliability of the BNI Screen for Higher Cerebral Functions for School-Age Children
George P. Prigatano, PhD
Saurabh Gupta, MC
Vicky T. Lomay, PhD
Division of Neurology, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Test-retest reliability of the total score obtained from the BNIS-C was examined in 25 children. The mean difference in scores between the two testing sessions was only one point. The correlation of BNIS-C Total scores obtained during the
first and second testing sessions was +.812. This preliminary study indicates that the BNIS-C Total score can be obtained reliably.
Key Words: reliability, BNI Screen for Higher Cerebral Function for School-Age Children, children
Abbreviations used: BNIS-C, BNI Screen for Higher Cerebral Function for School-Age Children; SD, standard deviation
The rationale and initial validation studies of the BNIS-C were recently reported.[5] As a part of the standardization study, the test-retest reliability of the BNIS-C Total score was examined. The goal of the study was to determine the stability of the BNIS-C Total score for children with no history of brain dysfunction.
Methods and Materials
Subjects
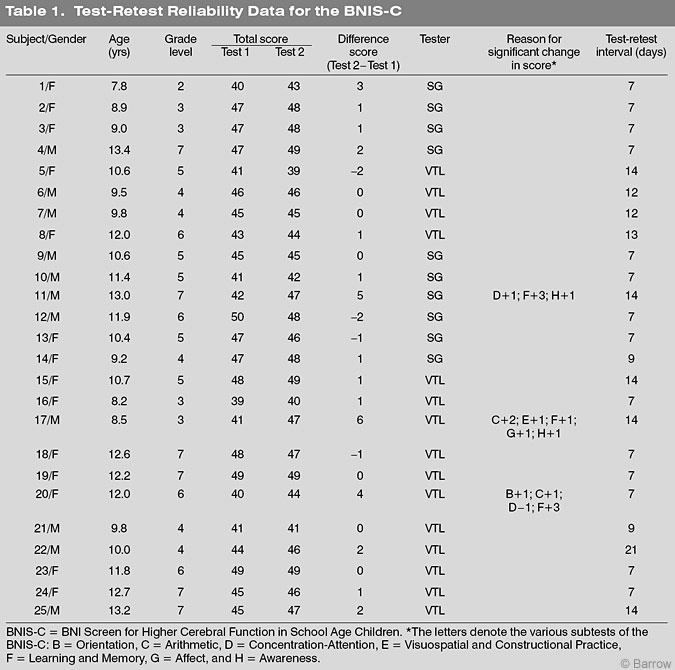
Twenty five school-age children (14 girls,11 boys) between the ages of 7 and 13 years (mean, 10.3 years; SD, 1.75; Table 1) were administered the BNIS-C on two separate occasions. All children attended public school in the central Phoenix area and were enrolled in the standardization study. All were in regular classes; none were receiving special education services.
Procedures
Two examiners (SG and VTL) independently tested and retested the 25 children. At the time of the first examination, the children were administered the BNIS-C and then three subtests of the Wechsler Intelligence Scale for Children-Fourth Edition.[8] They were also administered the Halstead Finger TappingTest[3] and a modification of the Fuld Object Memory Test.[2] At the second testing session, only the BNIS-C was administered.
The interval between the first and second sessions ranged from 7 to 21 days. The mean interval was 9.76 days (SD=3.79).
The time required to complete testing for the first testing session was about 1 hour. The time to complete testing for the second session was about 15 minutes. For each subject for both sessions, the BNIS-C Total scores, mean differences, and range of difference scores were calculated. The Pearson product moment correlation was used to estimate the test-retest reliability index (or coefficient).
Results
Table 1 lists each subject’s age, grade level in school, gender, and total BNIS-C score for the first and second testing sessions. The mean Total score on the BNIS-C during the first test session was 44.68 points (SD=3.28). The mean score during the second test session was 45.72 points (SD=2.87). The mean difference score between the two sessions was about 1 point. The difference in the BNIS-C Total score between the two test sessions was within 2 points in 21 (84%) of the 25 children. The difference score was three points in one child. Together, these children constitute 88% of the sample. Three (12%) children, respectively, had scores that were 4, 5, and 6 points higher on the second examination.
For the children whose Total score was 4 or more points higher on the second test, the differences primarily appeared to reflect improvements in their memory (F subtest) and awareness scores (H subtest). Some children tended to perform higher on arithmetic (C subtest) during the second examination compared to the first examination.
The Pearson product moment between scores on the first and second test session correlation was r =+.821, p=.000,n=25.
Discussion
The test-retest reliability of the BNIS-C Total score was acceptable for school-age children (r =+.821) but less than what was observed in adults who have taken the BNIS (r =+.94).[7] Baron[1] has emphasized the importance (and at times the difficulties) of sustaining a child’s test-taking behavior. To obtain a reliable performance,examiners must be vigilant to ensure that a child is adequately engaged in a psychometric task. In the present study, a reliable performance appeared to be obtained in 88% of the children who were retested. Children 11 and 20, whose BNIS-C Total scores increased substantially between the two test sessions, were 13 and 12 years old, respectively. Our normative data suggest that an expected mean score is 46.3 points for 13-year-olds and 45.5 points for 12-year-olds. These two children’s scores during the first test session were substantially lower than the normative estimates.Their second test scores were close to expected performance. Consequently, these children may not have been adequately engaged during the first test session.
When children are examined and their BNIS-CTotal score is less than expected for their age range,the examiner should be especially vigilant to determine if they were performing adequately when they have no history of known brain dysfunction or learning disability. In schoolage children of average intelligence with no history of brain dysfunction and no change in clinical status, the BNIS-C Total score typically should be within±2 points on any given test session. These findings re-emphasize the importance of having experienced examiners administer the BNIS-C to obtain reliable results.[6]
Interestingly, the children’s performance did not substantially differ on language tests or on tasks involving visuospatial skills. This finding may be of clinical significance given that performance on these subtests appears to be affected negatively after moderately severe to severe traumatic brain injury.[4] If children’s performance on these subtests substantially improves, the change may reflect an actual change in their clinical status. Future studies will be needed to assess this possibility.
Acknowledgment
This study was made possible in part by funds from the Newsome Chair in Neuropsychology to the senior author.
References
- Baron IS: Neuropsychological Evaluation of the Child. New York: Oxford University Press, 2004
- Fuld PA: Fuld Object-Memory Evaluation. Wood Dale, Illinois: Stoelting, 1981
- Halstead WC: Brain and Intelligence. Chicago: University of Chicago Press, 1947
- Prigatano GP: Community and school re-integration after childhood traumatic brain injury. Course Handouts, American Academy of Physical Medicine and Rehabilitation, pp 151-165, 2004
- Prigatano GP: The BNI Screen for children: Rationale and initial validation studies. Barrow Quarterly 20(2):27-32, 2004
- Prigatano GP, Amin K, Rosenstein LD: Administration and Scoring Manual for the BNI Screen for Higher Cerebral Functions. Phoenix, Arizona: Barrow Neurological Institute, 1995
- Rosenstein LD, Prigatano GP, Amin K: Reliability studies for the BNI Screen for Higher Cerebral Functions. BNI Quarterly 8(3):24-28, 1992
- Wechsler D: Wechsler Intelligence Scale for Children. Administration and Scoring Manual. San Antonio, Texas: The Psychological Corporation, 2003