
The Middle Fossa Approach
Authors
Fernando L. Gonzalez, MD
Mauro A. T. Ferreira, MD
Joseph M. Zabramski, MD
Robert F. Spetzler, MD
Pushpa Deshmukh, PhD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
The internal auditory canal can be approached through the middle fossa by following anatomic landmarks. Cadaveric dissections are used to illustrate the anatomy relevant to this surgery. The middle fossa approach is a useful option for small lesions when hearing might be preserved. The approach is versatile because it can be extended anteriorly by drilling the petrous apex (Kawase’s triangle) and gaining access to the posterior fossa and petroclival area.
Key Words: acoustic neuromas, facial nerve, middle fossa approach, petrosectomy
The middle fossa approach, as popularized by William House, provides excellent exposure to the internal auditory canal (IAC) for the removal of small acoustic tumors with the potential for hearing preservation. The anterior extension of this approach described by Kawase enhances the surgical exposure provided by this route to the upper clivus and petrous apex. This article focuses on the most relevant anatomical and technical aspects involved with accessing the IAC and with removing the petrous apex when greater exposure is needed.
Middle Fossa Approach
In 1904 Parry[16] first described the middle fossa approach for vestibular nerve section. At that time exposure of this nerve was associated with a high rate of morbidity. In 1961 William House, an eye, nose, and throat surgeon working with Dr. Theodore Kurze, a neurosurgeon, revisited this surgical approach. They performed 14 cadaveric dissections and described the approach for decompression of the IAC for the treatment of otosclerosis.[8] The technique was abandoned, but its utility for removing acoustic neuromas was evident.[9]
Compared to other approaches to the IAC, the middle fossa approach adequately exposes the facial (CN VII) and superior vestibular nerves within the IAC. It permits exposure of the subarachnoid, intracanalicular, and labyrinthine segments, and the first portion of the horizontal (tympanic) segment of CN VII. It is useful for removing small lesions (up to 2 cm in diameter), primarily intracanalicular, with minimal extension into the posterior fossa. Depending on the size of a lesion, the possibility for preserving hearing with the middle fossa approach is good. It is useful whenever the above segments of CN VII need to be decompressed. Because the approach is from the superior surface of the temporal bone, the risk of inadvertently opening the posterior semicircular canal is less than that associated with the retrosigmoid approach, which involves drilling the posterior wall of the IAC.
The suboccipital retrosigmoid and the translabyrinthine approaches can also be used to expose the IAC. When the suboccipital approach is used, the ability to preserve hearing depends on the size of the lesion. If the tumor is less than 2 cm, the chance to preserve hearing is 53% but increases to 83% if the lesion is 1 cm or less.[17] The most important advantage of the suboccipital approach is that it can be used for lesions of different sizes. The trans labyrinthine approach is useful for intracanalicular lesions.
Its main drawback is that hearing must be sacrificed. A partial labyrinthectomy (that removes the superior and posterior semicircular canals), however, may preserve hearing.[18] In a recent study,[7] hearing was preserved in 100% of patients who underwent a “transcrusal” approach, in which only the superior and posterior semicircular canals, starting at the common crus, were removed. Bone removal to expose the IAC is also time consuming and requires in depth knowledge of the anatomy of the temporal bone. If a cerebrospinal fluid fistula occurs, it is harder to treat than with other approaches. The IAC can also be exposed by combining these three approaches (Table 1).
Relevant Anatomic Structures
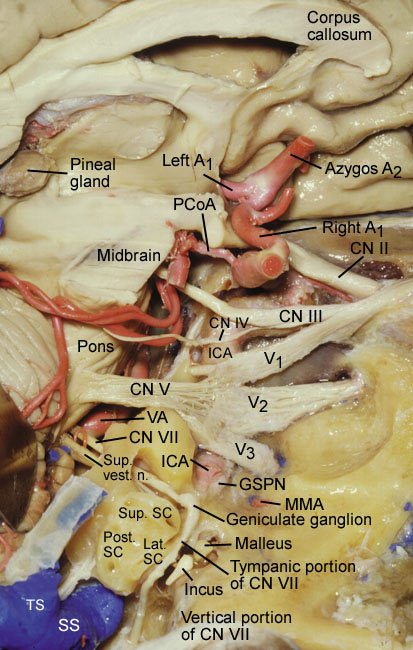
The ultimate goal of the middle fossa approach is to expose the IAC from above, from the roof of the petrous temporal bone. Although the IAC is not a middle fossa structure, its location (Fig. 1) is easily identified by the following important landmarks.
The internal maxillary artery, one of the two terminal branches of the external carotid artery, gives rise to the middle meningeal artery. The middle meningeal artery enters the cranium through the foramen spinosum and has two branches, the anterior and the posterior. The middle fossa approach involves the posterior branch.
The foramen spinosum is the outermost lateral structure in the middle fossa. According to de Oliveira et al.,5 the foramen spinosum is 4.7 mm in diameter and 2.5 to 8.0 mm anterolateral to the carotid canal. The third branch of the trigeminal nerve, the mandibular nerve (V3), is 2 to 3 mm medial to the foramen.
Typically, the tensor tympani muscle is roofed by bone. The muscle originates from the cartilaginous part of the eustachian tube and inserts via a tendon on the handle of the malleus. It is innervated by a tympanic branch of V3. When the muscle contracts, it tenses the tympanic membrane (hence its name), facilitating the ability to hear high-frequency tones.
The greater superior petrosal nerve (GSPN) is the first branch of CN VII and is composed of the latter’s preganglionic parasympathetic fibers. Originating from the geniculate ganglion, the GSPN travels in the floor of the middle fossa under the dura in the sphenopetrosal groove and can be either partially covered or not covered at all by bone. It is medial to the lesser petrosal nerve and could easily be mistaken for the latter.19 Hence, nerve stimulation can help identify the GSPN.[2]
Distal to the Gasserian ganglion, the GSPN lies at the anterior part of the foramen lacerum. There, it is joined by the deep petrosal nerve, which is composed of the sympathetic fibers from the pericarotid plexus. The deep petrosal nerve unites with the GSPN to become the vidian nerve. From the vidian canal, the vidian nerve courses to the sphenopalatine ganglion in the pterygopalatine fossa,[1] supplying post ganglionic fibers to the lacrimal glands.
The lesser petrosal nerve is com posed of parasympathetic fibers that originate in the inferior salivatory nucleus. It is a branch of the glossopharyngeal (CN IX) nerve and travels lateral to the GSPN in the same direction in the floor of the middle fossa under the dura.[19] It exits the foramen ovale directly to the otic ganglion where it joins a branch of V3, the auriculotemporal nerve, which innervates the parotid gland.
The petrosal segment (C3) of the internal carotid artery (ICA) enters the skull base through the carotid canal. The tympanic muscle is the landmark for identifying the genu of the ICA. After its genu, the ICA courses horizontally toward the petrous apex. A venous plexus and a network of sympathetic fibers surround the artery, from which exit two inconsistent branches. The caroticotympanic branch goes to the tympanic region (anterior and lateral to the genu of the petrosal ICA), and the vidian or pterygoid branch typically arises from the middle meningeal artery.[5]
PATIENT PORTALTRANSFER A PATIENTGET A SECOND OPINIONTHE BARROW NEUROPLEXFIND A DOCTORINTERNATIONAL PATIENTSCONTACT USPATIENTS & FAMILIESEDUCATIONRESEARCHDEPARTMENTS & PEOPLENEWS & STORIES
EducationGrand Rounds, Publications, & MediaBarrow QuarterlyVolume 16, No. 4, 2000The Middle Fossa Approach
- Aa Font Size
The Middle Fossa Approach
Authors
Fernando L. Gonzalez, MD
Mauro A. T. Ferreira, MD
Joseph M. Zabramski, MD
Robert F. Spetzler, MD
Pushpa Deshmukh, PhD
Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Abstract
The internal auditory canal can be approached through the middle fossa by following anatomic landmarks. Cadaveric dissections are used to illustrate the anatomy relevant to this surgery. The middle fossa approach is a useful option for small lesions when hearing might be preserved. The approach is versatile because it can be extended anteriorly by drilling the petrous apex (Kawase’s triangle) and gaining access to the posterior fossa and petroclival area.
Key Words: acoustic neuromas, facial nerve, middle fossa approach, petrosectomy
The middle fossa approach, as popularized by William House, provides excellent exposure to the internal auditory canal (IAC) for the removal of small acoustic tumors with the potential for hearing preservation. The anterior extension of this approach described by Kawase enhances the surgical exposure provided by this route to the upper clivus and petrous apex. This article focuses on the most relevant anatomical and technical aspects involved with accessing the IAC and with removing the petrous apex when greater exposure is needed.
Middle Fossa Approach
In 1904 Parry[16] first described the middle fossa approach for vestibular nerve section. At that time exposure of this nerve was associated with a high rate of morbidity. In 1961 William House, an eye, nose, and throat surgeon working with Dr. Theodore Kurze, a neurosurgeon, revisited this surgical approach. They performed 14 cadaveric dissections and described the approach for decompression of the IAC for the treatment of otosclerosis.[8] The technique was abandoned, but its utility for removing acoustic neuromas was evident.[9]
Compared to other approaches to the IAC, the middle fossa approach adequately exposes the facial (CN VII) and superior vestibular nerves within the IAC. It permits exposure of the subarachnoid, intracanalicular, and labyrinthine segments, and the first portion of the horizontal (tympanic) segment of CN VII. It is useful for removing small lesions (up to 2 cm in diameter), primarily intracanalicular, with minimal extension into the posterior fossa. Depending on the size of a lesion, the possibility for preserving hearing with the middle fossa approach is good. It is useful whenever the above segments of CN VII need to be decompressed. Because the approach is from the superior surface of the temporal bone, the risk of inadvertently opening the posterior semicircular canal is less than that associated with the retrosigmoid approach, which involves drilling the posterior wall of the IAC.
{kind=link}
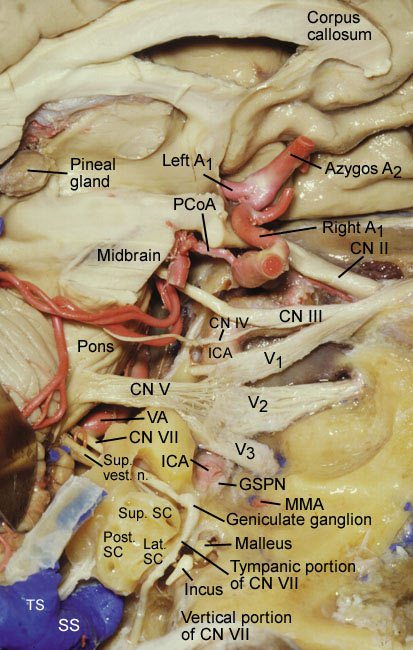
Figure 1. Primary anatomic structures of the middle fossa. The right cerebral hemisphere is removed and the dura of the middle fossa is peeled away. The middle meningeal artery (MMA) is exposed where it emerges from the foramen spinosum. The greater superior petrosal nerve (GSPN) is visible from the geniculate ganglion to the point where it courses below the mandibular branch of CN V. The geniculate ganglion is shown as well as the labyrinthine, tympanic, and subarachnoid portions of the facial nerve. A1, A2=segments of anterior cerebral artery, CN=cranial nerve, ICA=internal carotid artery, PCoA=posterior communicating artery, SC=semicircular canals, SS=sigmoid sinus, TS=transverse sinus, V1, V2, V3=branches of CN V,VA=vertebral artery.
The suboccipital retrosigmoid and the translabyrinthine approaches can also be used to expose the IAC. When the suboccipital approach is used, the ability to preserve hearing depends on the size of the lesion. If the tumor is less than 2 cm, the chance to preserve hearing is 53% but increases to 83% if the lesion is 1 cm or less.[17] The most important advantage of the suboccipital approach is that it can be used for lesions of different sizes. The trans labyrinthine approach is useful for intracanalicular lesions.
Its main drawback is that hearing must be sacrificed. A partial labyrinthectomy (that removes the superior and posterior semicircular canals), however, may preserve hearing.[18] In a recent study,[7] hearing was preserved in 100% of patients who underwent a “transcrusal” approach, in which only the superior and posterior semicircular canals, starting at the common crus, were removed. Bone removal to expose the IAC is also time consuming and requires in depth knowledge of the anatomy of the temporal bone. If a cerebrospinal fluid fistula occurs, it is harder to treat than with other approaches. The IAC can also be exposed by combining these three approaches (Table 1).
Relevant Anatomic Structures
The ultimate goal of the middle fossa approach is to expose the IAC from above, from the roof of the petrous temporal bone. Although the IAC is not a middle fossa structure, its location (Fig. 1) is easily identified by the following important landmarks.
The internal maxillary artery, one of the two terminal branches of the external carotid artery, gives rise to the middle meningeal artery. The middle meningeal artery enters the cranium through the foramen spinosum and has two branches, the anterior and the posterior. The middle fossa approach involves the posterior branch.
The foramen spinosum is the outermost lateral structure in the middle fossa. According to de Oliveira et al.,5 the foramen spinosum is 4.7 mm in diameter and 2.5 to 8.0 mm anterolateral to the carotid canal. The third branch of the trigeminal nerve, the mandibular nerve (V3), is 2 to 3 mm medial to the foramen.
Typically, the tensor tympani muscle is roofed by bone. The muscle originates from the cartilaginous part of the eustachian tube and inserts via a tendon on the handle of the malleus. It is innervated by a tympanic branch of V3. When the muscle contracts, it tenses the tympanic membrane (hence its name), facilitating the ability to hear high-frequency tones.
The greater superior petrosal nerve (GSPN) is the first branch of CN VII and is composed of the latter’s preganglionic parasympathetic fibers. Originating from the geniculate ganglion, the GSPN travels in the floor of the middle fossa under the dura in the sphenopetrosal groove and can be either partially covered or not covered at all by bone. It is medial to the lesser petrosal nerve and could easily be mistaken for the latter.19 Hence, nerve stimulation can help identify the GSPN.[2]
Distal to the Gasserian ganglion, the GSPN lies at the anterior part of the foramen lacerum. There, it is joined by the deep petrosal nerve, which is composed of the sympathetic fibers from the pericarotid plexus. The deep petrosal nerve unites with the GSPN to become the vidian nerve. From the vidian canal, the vidian nerve courses to the sphenopalatine ganglion in the pterygopalatine fossa,[1] supplying post ganglionic fibers to the lacrimal glands.
The lesser petrosal nerve is com posed of parasympathetic fibers that originate in the inferior salivatory nucleus. It is a branch of the glossopharyngeal (CN IX) nerve and travels lateral to the GSPN in the same direction in the floor of the middle fossa under the dura.[19] It exits the foramen ovale directly to the otic ganglion where it joins a branch of V3, the auriculotemporal nerve, which innervates the parotid gland.
The petrosal segment (C3) of the internal carotid artery (ICA) enters the skull base through the carotid canal. The tympanic muscle is the landmark for identifying the genu of the ICA. After its genu, the ICA courses horizontally toward the petrous apex. A venous plexus and a network of sympathetic fibers surround the artery, from which exit two inconsistent branches. The caroticotympanic branch goes to the tympanic region (anterior and lateral to the genu of the petrosal ICA), and the vidian or pterygoid branch typically arises from the middle meningeal artery.[5]
{kind=link}
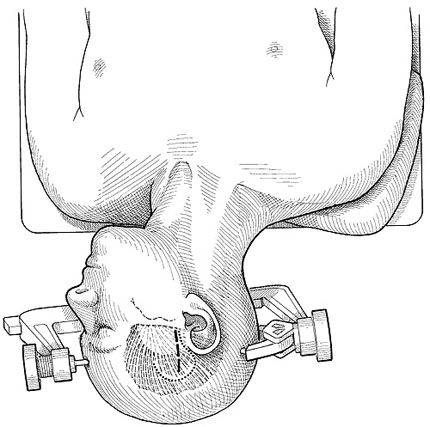
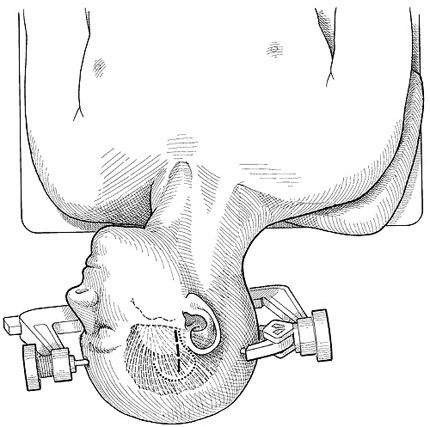
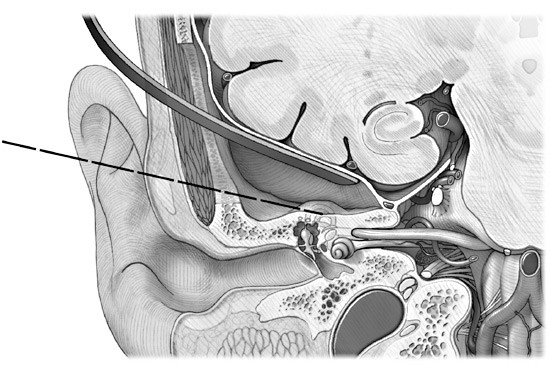
Figure 2. Skin incision for the middle fossa approach (dashed line). The patient’s head is rotated 90º to the contralateral side. A vertical incision begins anterior to the ear at the level of the zygomatic arch. A question mark incision (dotted line) is preferred when anterior extension is desired (e.g., transKawase approach) and reaching the petrous apex is the goal.
The cochlea is located in the axilla between the GSPN and facial nerve just below the geniculate ganglion.
The arcuate eminence is a bony prominence, formed by the superior semi circular canal in the floor of the middle fossa. Its location is too inconsistent to serve as an accurate landmark for localizing the superior semicircular canal.
The superior petrosal vein, also known as Dandy’s vein, is a part of the superficial draining system of the cerebellum on its petrosal surface and drains into the superior petrosal sinus. It is formed by the transverse pontine vein, the pontotrigeminal vein, the vein of the middle cerebellar peduncle, and the vein of the cerebellomedullary fissure.[15] The superior petrosal vein is not a structure of the middle fossa, but is important during surgery of the cerebellopon tine angle. When the middle fossa approach must be extended anteriorly, surgeons must be aware of this vein and its tributaries.
Surgical Technique
The long axis of the head is positioned parallel to the floor with the ear facing the ceiling and the neck slightly extended. A vertical incision, 5 to 6 cm long, is made anterior to the tragus and perpendicular to the zygomatic arch (Fig. 2). Fascia and temporal muscle are exposed and split with the Bovie electrocautery device and then retracted with a self-retaining retractor or fishhooks. A square-shaped craniotomy is performed. The squamous suture, which is a good landmark for identifying the superior limit of the craniotomy, is exposed.

A third of the craniotomy is positioned posterior and two-thirds of it anterior to the external auditory canal (Fig. 3) This configuration adequately exposes the floor of the middle fossa. Sometimes part of the temporal rim must be removed to obtain a flat exposure and thus minimize retraction of the temporal lobe (Fig. 4).
The dura is elevated posteriorly to anteriorly to prevent injury to the GSPN (Fig. 5). The GSPN and lesser petrosal nerve are just beneath the dura and become visible once it is elevated. Both nerves are delicate and the operating microscope must be used to identify them. The two nerves can be distinguished by electrical stimulation as mentioned earlier. When the dura is retracted medially, the middle meningeal artery, with its anterior and posterior branches, can be seen emerging from the foramen spinosum. The middle meningeal artery is sectioned just after it exits the foramen spinosum, which is then exposed along with V3.
In the posterior part of the exposure near the petrous ridge, the arcuate eminence becomes visible. The angle between the arcuate eminence and the GSPN is approximately 120º. After the GSPN, arcuate eminence, and petrous ridge are identified, the IAC can be localized by any of the following three techniques.
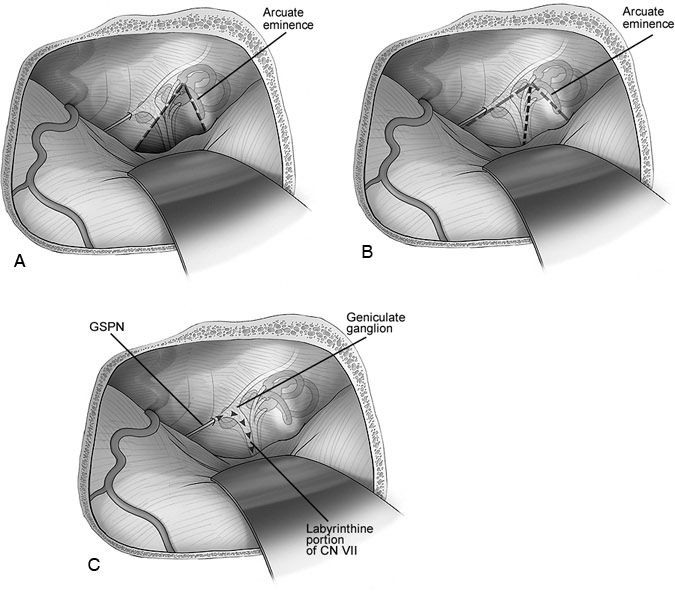
Fisch Technique. A line is drawn over the long axis of the arcuate eminence (Fig. 6A). Another line is drawn 60º to the first line away from the arcuate eminence. The second line provides the location of the IAC, which typically is 3 to 4 mm below the petrous ridge.[4] It has, however, been reported to be as much as 7 mm below the floor of the middle fossa.[11]
Garcia-Ibañez Technique. This technique (Fig. 6B) relies on the important relationship between the GSPN and the arcuate eminence, which are separated by 120º. Bisecting this angle provides the site at which to start drilling the temporal bone to expose the IAC.[6]
House Technique. House proposed that once the GSPN has been identified, it is possible to drill the floor of the middle fossa (2 to 3 mm), to identify the geniculate ganglion, and to follow the facial (labyrinthine portion) nerve medially until the IAC is reached (Fig. 6C).[6,8] The junction between the geniculate ganglion and the facial nerve is not on the same plane as the IAC but rather is slightly posterior. Therefore, most of the geniculate ganglion must be unroofed to expose the facial nerve medially.
After the roof of the IAC has been drilled (3 to 4 mm below the floor of the middle fossa), the vertical bar of bone (also known as Bill’s bar in honor of Dr. William House) is easily identified. This bar separates the facial nerve from the superior vestibular nerve. Adjacent to the IAC is the meatal portion of the anterior inferior cerebellar artery (AICA), which forms an important loop, sometimes enters the IAC, and then passes through the nerves. The anatomy of the AICA in this region is quite variable as is the percentage of its loop located inside the IAC. According to Martin et al.,14 54% of meatal segments protrude into the IAC.
The internal auditory artery sends branches to the bone and dura lining the IAC. According to Martin et al. the internal auditory artery emerged from the premeatal segment in 77% of their anatomical specimens, from the meatal segment in 21%, and from the post meatal segment in 2%. This artery also can emerge outside or at the meatus.14 Its patency is a prerequisite to the preservation of hearing.
The recurrent artery is also important because it supplies blood to the pons, middle cerebellar peduncle, and the entry zone of the trigeminal nerve (CN V). It can be found between or anterior, anteroinferior, or superior to the facial and vestibular nerves.14 Early identification and preservation of these arterial branches inside the IAC are fundamental to the preservation of hearing during the resection of acoustic neuromas.
Extended Middle Fossa Approach to the IAC and Clivus
Despite the excellent exposure of the IAC afforded by the traditional middle fossa approach, it is inadequate for the removal of tumors that extend into the posterior fossa or lesions in the petroclival region. To resect tumors with such medial extensions, a wider approach is needed.
Kawase’s group[10] first described an area of the temporal bone that can be removed with impunity. For the treatment of low-neck basilar tip aneurysms (between the sellar floor and IAC on a lateral projection), they described an approach that later proved useful for resecting meningiomas of the petroclival region.[3,12,13] In 1986 Day et al.[4] developed a geometric construct by compartmentalizing structures in and adjacent to the cavernous sinus. They named the area described by Kawase as the posteromedial triangle and its limits were as follows: the porustrigeminus, cochlea, and posterior border of the mandibular branch (Fig. 7).[6] The triangle is devoid of any vascular or nerve branches and limited by the margin of V3, the petrous ridge, the GSPN laterally, and the nerves inside the IAC posteriorly. The principle of this approach is the same as for the middle fossa. Hence, early identification of the IAC is important.
Surgical Technique
The head is positioned as described for the traditional middle fossa approach. The incision is in the shape of an inverted question mark big enough to include the squamous portion of the temporal bone and part of sphenotemporal bone (Fig. 2). Below the skin incision, the fascia is incised in a semicircular fashion. The craniotomy must include the sphenotemporal junction, and its position varies depending on if it needs to be extended anteriorly enough to include the posterior part of cavernous sinus.
The petrous apex is exposed extradurally until the petrous ridge is identified. The dura is again elevated posteriorly to anteriorly, and the foramen spinosum is identified. The middle meningeal artery is coagulated so that the dura can be elevated and V3 visualized. The petrosal nerves are located medially, just under the dura.
To expose the IAC, the superior petrosal sinus and petrous ridge must be identified. An incision is made above and below the ridge so that the sinus can be ligated just posterior to the porus trigeminus. The sinus must be ligated before the entry point of the superior petrosal vein so that it will drain normally into the transverse sinus. Utmost care must be exercised to protect the trochlear nerve (CN IV), which courses just below the tentorium and can be easily damaged. After V3, GSPN, and CN VII and the vestibulocochlear nerve (CN VIII) have been identified in the IAC and the superior petrosal sinus has been ligated, this piece of bone, which is devoid of important structures, can be drilled until the dura of the posterior fossa becomes visible (Fig. 8).
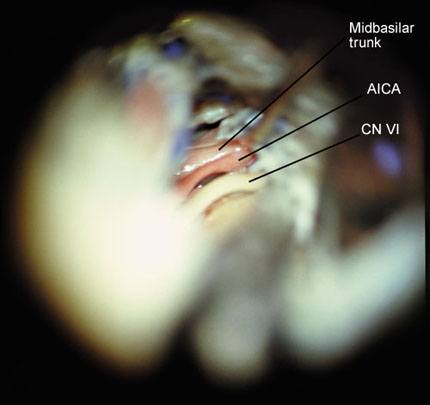
In this exposure the basilar trunk, the emergence of the AICA, and abducens nerve are visible medially (Fig. 9) and the nerves inside the IAC are visible posteriorly. The brain stem is exposed from the pontomedullary sulcus, and the anterolateral portion of the pons between CN V and CN VII is also visible.
Conclusions
The middle fossa approach is an option for the removal of small acoustic neuromas (inside the internal auditory canal). It is adequate for the decompression of CN VII and provides the landmarks associated with exposure of the petrous portion of the ICA when a bypass (C3-C5) is needed. The anterior extension (transKawase) provides an excellent option for petroclival lesions, lesions of the middle third of the clivus, and AICA aneurysms. This complicated anatomy must be mastered by practicing anatomical dissection and drilling of the temporal bone.
References
- Brazis PW, Masdeu JC, Biller J: The localization of lesions affecting cranial nerve VII (the facial nerve), in Brazis PW, Masdeu JC, Biller J (eds): Localization in Clinical Neurology. Boston: Little, Brown and Company, 1996, pp 271-291
- Chicoine MR, van Loveren HR: Surgical approaches to the cavernous sinus, in Robertson JT, Coakham HB, Robertson JH (eds): Cranial Base Surgery. London: Churchill Livingstone, 2000, pp 171-185
- David CA, Spetzler RF: Petroclival meningiomas. BNI Quarterly 15(2):4-14, 1999
- Day JD, Fukushima T, Giannotta SL: Microanatomical study of the extradural middle fossa approach to the petroclival and posterior cavernous sinus region: Description of the rhomboid construct. Neurosurgery 34:1009-1016, 1994
- de Oliveira E, Tedeschi H, Rhoton AL, Jr., et al: Microsurgical anatomy of the internal carotid artery: Intrapetrous, intracavernous, and clinoidal segments, in Carter LP, Spetzler RF (eds): Neuro vascular Surgery. New York: McGraw-Hill, 1995, pp 3-10
- Fukushima T, Day JD: Manual of Skull Base Dissection. Pittsburgh: AF NeuroVideo, 1996
- Horgan MA, Anderson GJ, Schwartz MS, et al: Classification and quantification of the petrosal approach (abst). Skull Base Surgery 10(suppl 1): 11, 2000
- House WF: Surgical exposure of the internal auditory canal and its contents through the middle cranial fossa. Laryngoscope 71:1363-1385, 1961
- House WF, Shelton C: Middle fossa approach for acoustic tumor removal. Otolaryngol Clin North Am 25:347-359, 1992
- Kanzaki J, Kawase T, Sano K, et al: A modified extended middle cranial fossa approach for acoustic tumors. Arch Otorhinolaryngol 217:119-121, 1977
- Kawase T, Shiobara R: Extended middle cranial fossa approaches to the clivus and acoustic meatus, in Torrens M, Al-Mefty O, Kobayashi S (eds): Operative Skull Base Surgery. New York: Churchill Livingstone, 1997, pp 263-278
- Kawase T, Shiobara R, Toya S: Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas: Surgical method and results in 10 patients. Neurosurgery 28:869-876, 1991
- Kawase T, Toya S, Shiobara R, et al: Transpetrosal approach for aneurysms of the lower basilar artery. J Neurosurg 63:857-861, 1985
- Martin RG, Grant JL, Peace D, et al: Microsurgical relationships of the anterior inferior cerebellar artery and the facial-vestibulocochlear nerve complex. Neurosurgery 6:483-507, 1980
- Matsushima T, Rhoton AL, Jr., de Oliveira E, et al: Microsurgical anatomy of the veins of the posterior fossa. J Neurosurg 59:63-105, 1983
- Parry RH: A case of tinnitus and vertigo treated by division of the auditory nerve. J Laryngol 19:402-406, 1904
- Post KD, Eisenberg MB, Catalano PJ: Hearing preservation in vestibular schwannoma surgery: What factors influence outcome? J Neurosurg 83:191-196, 1995
- Sekhar LN, Schessel DA, Bucur SD, et al: Partial labyrinthectomy petrous apicectomy approach to neoplastic and vascular lesions of the petroclival area. Neurosurgery 44:537-552, 1999
- Wilson-Pauwels L, Akesson EJ, Stewart PA: Glossopharyngeal nerve, in Wilson-Pauwels L, Akesson EJ, Stewart PA (eds): Cranial Nerves. Anatomy and Clinical Comments. Toronto: B.C. Decker, 1988, pp 114-123